
The Flexor Hallucis Longus in Ankle Sprain Mechanics
Why the Big Toe Flexor Matters for Foot Function, Propulsion, and Recovery
Ankle sprains are among the most common musculoskeletal injuries worldwide. In sport alone they account for up to 40% of all athletic injuries, with the majority involving the lateral ankle ligaments during inversion events (Fong et al., 2007; Doherty et al., 2014).

Flexor Hallucis Longus and Ankle Sprains: Why Big Toe Mechanics Matter for Foot Function Canberra | The Body Lab
Clinically, most rehabilitation protocols focus on restoring ligament stability, proprioception, and peroneal muscle strength. While these components are important, this perspective may overlook the broader biomechanical system of the foot and ankle.
The ankle does not operate in isolation. It functions as part of a coordinated propulsion system linking the lower limb to the ground.
Within this system lies a structure that is frequently overlooked in ankle injury discussions: the Flexor Hallucis Longus (FHL).
The FHL is a long tendon connecting the posterior lower leg to the tip of the big toe. Traditionally it has received attention primarily in dancers due to overuse injuries associated with pointe work (Wentzell, 2018). However, its potential involvement in ankle sprain mechanisms and post-injury dysfunction is less widely discussed.
Given the anatomical proximity of the FHL to the ankle joint and its functional role in propulsion, arch stability, and force transmission, the tendon may play a far greater role in ankle injury recovery than is currently recognised.
This paper explores the anatomical, biomechanical, and clinical relevance of the FHL in ankle sprains and considers its implications for movement-based rehabilitation.
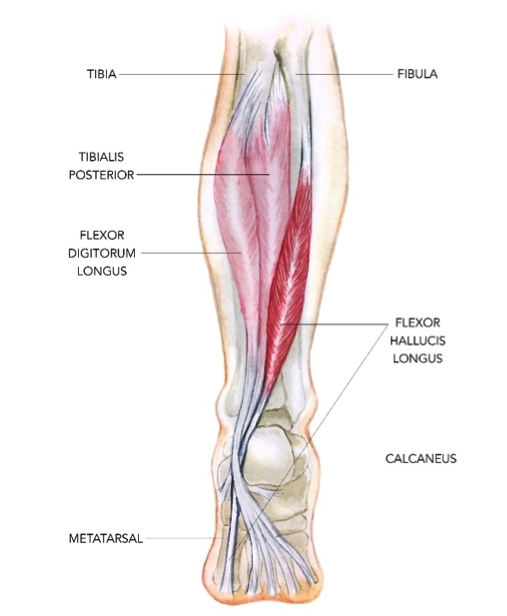
Anatomy of the Flexor Hallucis Longus
The Flexor Hallucis Longus originates from the posterior surface of the distal two-thirds of the fibula and the adjacent interosseous membrane.
From its muscular origin, the tendon travels distally through a complex anatomical path involving several key mechanical structures.
Posterior ankle tunnel
At the ankle, the tendon enters the deep posterior compartment, travelling alongside two other tendons:
• Tibialis Posterior
• Flexor Digitorum Longus
• Flexor Hallucis Longus
This trio is commonly remembered by anatomy students as “Tom, Dick and Harry.”
However, the FHL sits slightly deeper and more lateral than the other two tendons. It passes through a fibro-osseous groove between the posterior talus and the sustentaculum tali, forming a narrow tunnel that can become a site of mechanical compression (Hamilton et al., 2008).
Midfoot crossing — the Knot of Henry
Further distally, the FHL tendon crosses the flexor digitorum longus tendon in the midfoot at the Knot of Henry.
Flexor Hallucis Longus and Ankle Sprains: Why Big Toe Mechanics Matter for Foot Function Canberra | The Body Lab
This region contains inter-tendinous connections that allow load sharing between the hallux and lesser toes, enabling coordinated toe flexion during locomotion.
Sesamoid pulley system
At the forefoot, the FHL passes between the medial and lateral sesamoid bones beneath the first metatarsal head before inserting onto the distal phalanx of the hallux.
These sesamoids act as pulleys, increasing the mechanical advantage of the tendon during toe flexion.
The result is a tendon that spans almost the entire length of the lower limb, linking:
posterior leg → ankle → midfoot → forefoot → big toe
This long anatomical path allows the FHL to play a role in multiple stages of locomotion.
Functional Role of the FHL in Human Movement
Although the primary action of the FHL is plantarflexion of the big toe, its functional role is far more extensive.
The tendon contributes to several key biomechanical processes during walking and running.
Hallux stabilisation during push-off
During late stance in gait, the hallux becomes the final point of contact with the ground.
At this stage the FHL contributes to:
• stabilising the first ray
• generating push-off force
• maintaining forefoot rigidity
Research has demonstrated that hallux function significantly influences propulsion mechanics, with restricted hallux motion reducing walking efficiency (Smith et al., 2021).
Dynamic support of the medial arch
The FHL also contributes to the dynamic stabilisation of the medial longitudinal arch.
As the hallux dorsiflexes during late stance, tension develops in the plantar fascia through the windlass mechanism, increasing arch stiffness (Hicks, 1954).
The FHL assists this process by:
• flexing the hallux
• stabilising the first metatarsal
• supporting arch tension
This mechanism transforms the foot from a flexible shock absorber into a rigid lever for propulsion.
Contribution to elastic energy storage
Human locomotion relies heavily on elastic energy storage in muscle-tendon units.
Studies of running mechanics show that the ankle plantarflexors store and release substantial elastic energy during gait, improving efficiency and reducing metabolic cost (Lai et al., 2014).
While the gastrocnemius–soleus complex plays the primary role, the FHL contributes to this elastic system by stabilising the forefoot during energy release.
Assistance in ankle plantarflexion
The FHL also assists ankle plantarflexion.
Although not a prime mover, it contributes to plantarflexion torque during the push-off phase of gait, working synergistically with the calf muscles.
The Mechanics of Ankle Sprain
The most common ankle sprain occurs when the foot undergoes:
plantarflexion combined with inversion
This motion typically produces:
tensile stress on the lateral ligaments
compressive stress on the medial and posterior ankle structures
While ligament injury receives most clinical attention, the compression forces generated in the posterior ankle region may affect structures such as:
• the posterior talus
• the posterior ankle capsule
• the Flexor Hallucis Longus tendon
Because the FHL passes through a tight tunnel behind the talus, it is vulnerable to compression or irritation during inversion injuries.
Mechanisms Linking the FHL to Ankle Sprain Injury
Several anatomical and biomechanical factors explain why the FHL may become involved in ankle injuries.
Posterior ankle compression
During plantarflexion, the posterior talus approximates surrounding structures.
This motion narrows the space within the posterior talar groove, increasing pressure on the FHL tendon.
In inversion injuries, this compression may occur rapidly and forcefully, potentially irritating the tendon.
This mechanism resembles the pathology seen in posterior ankle impingement syndrome, where the FHL is frequently involved (Hamilton et al., 2008).
Tendon sheath communication with the ankle joint
Anatomical studies have demonstrated that the FHL tendon sheath sometimes communicates directly with the ankle joint capsule (Dalmau-Pastor et al., 2015).
When this occurs, joint effusion following ankle sprain may extend into the tendon sheath, producing FHL tenosynovitis.
This phenomenon may explain why some patients experience persistent posteromedial ankle pain after ligament healing.
Altered loading after injury
Following ankle sprain, individuals often develop compensatory gait patterns.
Common changes include:
• reduced push-off
• altered forefoot loading
• restricted hallux motion
These changes can shift mechanical load onto the FHL tendon, particularly during late stance.
Over time this altered loading pattern may contribute to ongoing irritation.
Clinical Indicators of FHL Involvement
When the FHL is involved in ankle injury, symptoms may differ from typical ligament pain.
Common clinical features include:
Posteromedial ankle pain
Pain is typically felt behind the ankle and slightly toward the inside of the joint.
Pain during push-off
Activities that load the forefoot often reproduce symptoms, including:
• running
• jumping
• calf raises
• uphill walking
Hallux movement pain
Resisted big toe flexion or passive extension may provoke discomfort.
Limited ankle dorsiflexion
Because the tendon wraps around the posterior ankle, irritation can contribute to restricted forward ankle movement.
Toe Strength and Athletic Performance
Beyond injury recovery, the hallux plays an important role in athletic performance.
Recent studies have demonstrated that toe flexor strength correlates with sprinting ability, jump performance, and agility (Mickle et al., 2016).
Toe strength has also been linked to:
• balance control
• fall prevention in older adults
• improved running economy
These findings highlight the importance of the hallux in transmitting force from the lower limb to the ground.
If the hallux cannot stabilise effectively, the entire propulsion system becomes less efficient.
Implications for Rehabilitation
Traditional ankle rehabilitation focuses primarily on:
• ligament healing
• proprioceptive training
• peroneal muscle strengthening
While these interventions are valuable, a more comprehensive approach should also consider hallux and forefoot mechanics.
Rehabilitation strategies may include:
restoring hallux mobility
Ensuring adequate range of motion at the first metatarsophalangeal joint.
strengthening toe flexors
Improving the capacity of the FHL and intrinsic foot muscles.
improving foot-ankle coordination
Encouraging coordinated motion between the forefoot, midfoot, and ankle.
reintegrating gait mechanics
Because propulsion involves the entire lower limb, rehabilitation should also address:
• calf strength
• hip extension mechanics
• running and walking technique
A Systems Perspective of Ankle Injury
An ankle sprain is rarely just a ligament injury.
It represents a disruption in the coordinated movement of the foot–ankle propulsion system.
The Flexor Hallucis Longus sits at a critical junction within this system, linking the posterior lower leg to the forefoot.
Due to its anatomical location and functional role in push-off mechanics, dysfunction of the FHL may contribute to:
• persistent ankle stiffness
• reduced propulsion power
• ongoing posteromedial ankle pain
• delayed return to sport
For clinicians working in movement therapy, sports rehabilitation, or biomechanics, evaluating the hallux and forefoot as part of ankle injury assessment may provide valuable insights.
Sometimes the difference between lingering symptoms and a full recovery comes down to whether a small but powerful tendon — running from the fibula to the tip of the big toe — is functioning as it should.