
Achilles Ruptures Are Rising
A 2026 systematic review by Kotsifaki et al. 2026 Achilles Tendon Rupture Study analysed over 70 years of global data on Achilles tendon ruptures, making it one of the most comprehensive datasets we have on this topic.
The conclusion is consistent and difficult to ignore:
Achilles tendon ruptures have increased significantly over the past six to seven decades.
This is not a small trend. It reflects a meaningful shift in how modern humans load, train, and use their lower limbs.
What the Study Found
The review pooled data across multiple decades and populations and identified several key patterns:
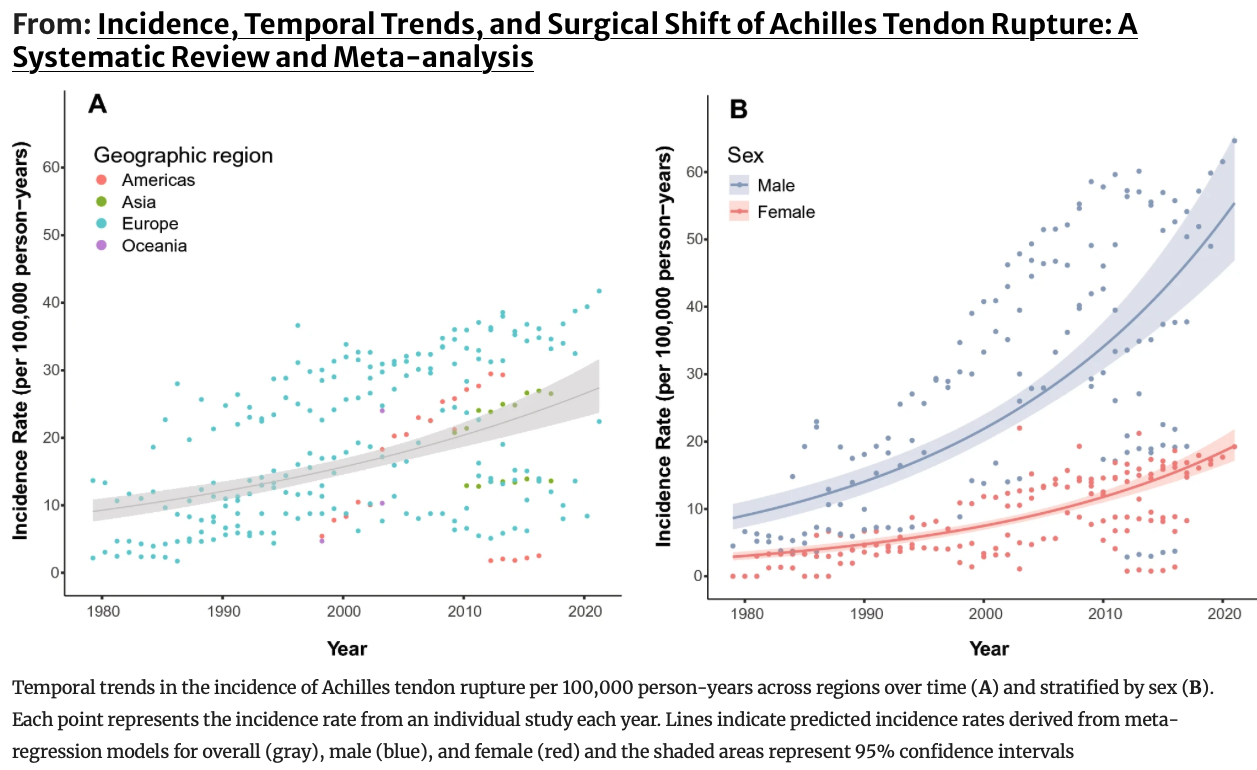
A progressive increase in incidence from the mid-20th century to present
Higher prevalence in men, particularly aged 30–50
A strong association with recreational sport participation
Approximately 65–70% of ruptures are sport-related
A decline in surgical intervention since the early 2000s, with increased reliance on structured rehabilitation
This aligns with earlier epidemiological studies showing similar trends in Europe and North America, where incidence rates have risen from approximately 2–5 per 100,000 to over 20 per 100,000 in some populations (Lantto et al., 2015; Huttunen et al., 2014).
Why This Is Happening
Reduced Tissue Capacity
Tendon tissue adapts to load through mechanotransduction—where mechanical stress stimulates cellular responses that increase collagen synthesis and structural integrity.
However, this process is slow and cumulative.
Research suggests that meaningful tendon adaptation requires weeks to months of consistent loading, with collagen remodelling continuing over even longer periods (Magnusson et al., 2010).
When activity levels increase rapidly—such as returning to sport, starting a new program, or increasing intensity—load exceeds capacity, and the tendon becomes vulnerable.
Sudden Load Exposure
Modern training patterns often involve intermittent exposure to high forces:
Social sport with unpredictable intensity
High-intensity interval training
Recreational sprinting or jumping
The Achilles tendon experiences forces up to 6–8 times body weight during running and even higher during sprinting (Komi, 1992; Lichtwark & Wilson, 2005).
Without progressive preparation, these loads create excessive strain within the tendon matrix, increasing the likelihood of micro-damage accumulation and eventual rupture.
Poor Load Distribution
The Achilles tendon is not designed to work in isolation.
It is part of an integrated kinetic chain involving:
The foot as a load-absorbing and force-transferring structure
The ankle joint as a rotational interface
The knee and hip as contributors to force generation and dissipation
When motion is restricted—particularly in the foot and ankle—force transmission becomes inefficient, and load is concentrated in fewer tissues.
This concept aligns with the idea of stress shielding and stress concentration, where reduced variability in movement leads to localized overload (Lieber & Ward, 2013).
Foot Function Limitations
The foot plays a central role in managing ground reaction forces.
During gait:
Pronation allows load absorption and energy dissipation
Supination creates a rigid lever for propulsion
First MTP joint extension engages the windlass mechanism, increasing arch stiffness
If these functions are limited:
Load absorption decreases
Propulsive efficiency reduces
The Achilles compensates by increasing tensile demand
Research on foot mechanics shows that reduced first metatarsophalangeal joint dorsiflexion and altered arch behaviour are associated with increased strain in the Achilles tendon (Caravaggi et al., 2009; Hicks, 1954).
Common Misconceptions
It Is Not Isolated
The Achilles tendon is often treated as a local structure, but its function is dependent on whole-limb coordination.
Studies on gait and running mechanics demonstrate that proximal control (hip and trunk) significantly influences distal loading patterns (Schache et al., 2012).
Treating the tendon without addressing upstream and downstream mechanics limits long-term outcomes.
Stretching Is Not Sufficient
While stretching may temporarily alter muscle-tendon length, it does not significantly improve tendon load capacity.
Effective tendon adaptation requires:
Mechanical loading
Time under tension
Progressive overload
Heavy slow resistance training has been shown to produce comparable or superior outcomes to eccentric-only programs in Achilles tendinopathy (Beyer et al., 2015).
Symptoms Precede Injury
Achilles ruptures are rarely truly spontaneous.
Most individuals report prior symptoms:
Morning stiffness
Localised tendon pain
Reduced performance or “tightness”
These signs reflect underlying tendon pathology, often involving collagen disorganisation and reduced mechanical integrity (Cook & Purdam, 2009).
Ignoring these signals increases the risk of progression toward rupture.
Clinical Implications
Progressive Loading
Tendon rehabilitation and preparation should follow a staged approach:
Isometric loading for early pain modulation
Heavy slow resistance to improve tendon capacity
Plyometric and elastic loading to restore energy storage and release
This progression reflects the continuum model of tendon adaptation.
Foot Mechanics
Restoring foot function reduces unnecessary load on the Achilles.
Key components include:
Arch mobility for load absorption
Ankle rotation for force transfer
First MTP joint extension for efficient propulsion
Improving these elements redistributes force across the system.
Load Management
The most important variable is not exercise selection—it is load progression.
Gradual increases in:
Volume
Intensity
Frequency
allow the tendon to adapt without exceeding its capacity.
Abrupt changes remain one of the strongest predictors of injury.
Conclusion
The increase in Achilles tendon ruptures reflects a broader issue in modern movement:
We are applying higher forces to systems that are underprepared to manage them.
The solution is not avoidance of load, but better preparation for load.
This includes:
Progressive tendon conditioning
Restoration of foot and ankle mechanics
Integration of whole-body movement patterns
When these elements are addressed, the Achilles tendon is not a weak link—it becomes one of the most powerful and efficient structures in human movement.
ReferencesKotsifaki R, Malisios P, Byron C, Marques J, Korakakis V.Incidence, Temporal Trends, and Surgical Shift of Achilles Tendon Rupture: A Systematic Review and Meta-analysis. Sports Medicine. 2026.Lantto I, Heikkinen J, Flinkkilä T, et al.Epidemiology of Achilles tendon ruptures: increasing incidence over time. Scand J Med Sci Sports. 2015.Huttunen TT, Kannus P, Rolf C, et al.Acute Achilles tendon ruptures: incidence of injury and surgery in Sweden. Am J Sports Med. 2014.Magnusson SP, Langberg H, Kjaer M.The pathogenesis of tendinopathy: balancing the response to loading. Nat Rev Rheumatol. 2010.Komi PV.Relevance of in vivo force measurements to human biomechanics. J Biomech. 1992.Lichtwark GA, Wilson AM.In vivo mechanical properties of the human Achilles tendon. J Exp Biol. 2005.Lieber RL, Ward SR.Tendon mechanics and pathophysiology. J Orthop Sports Phys Ther. 2013.Caravaggi P, et al.Functional role of the plantar fascia during gait. J Biomech. 2009.Hicks JH.The mechanics of the foot: The plantar aponeurosis and the arch. J Anat. 1954.Schache AG, Dorn TW, Williams GP, Brown NAT, Pandy MG.Lower-limb muscular strategies for increasing running speed. J Orthop Sports Phys Ther. 2012.Beyer R, et al.Heavy slow resistance versus eccentric training in Achilles tendinopathy. Am J Sports Med. 2015.Cook JL, Purdam CR.Is tendon pathology a continuum? Br J Sports Med. 2009.