
Pes Planus vs Pes Cavus: How Foot Shape May Alter Nerve Stress and Contribute to Heel Pain
Pes Planus vs Pes Cavus: How Foot Shape May Alter Nerve Stress and Contribute to Heel Pain
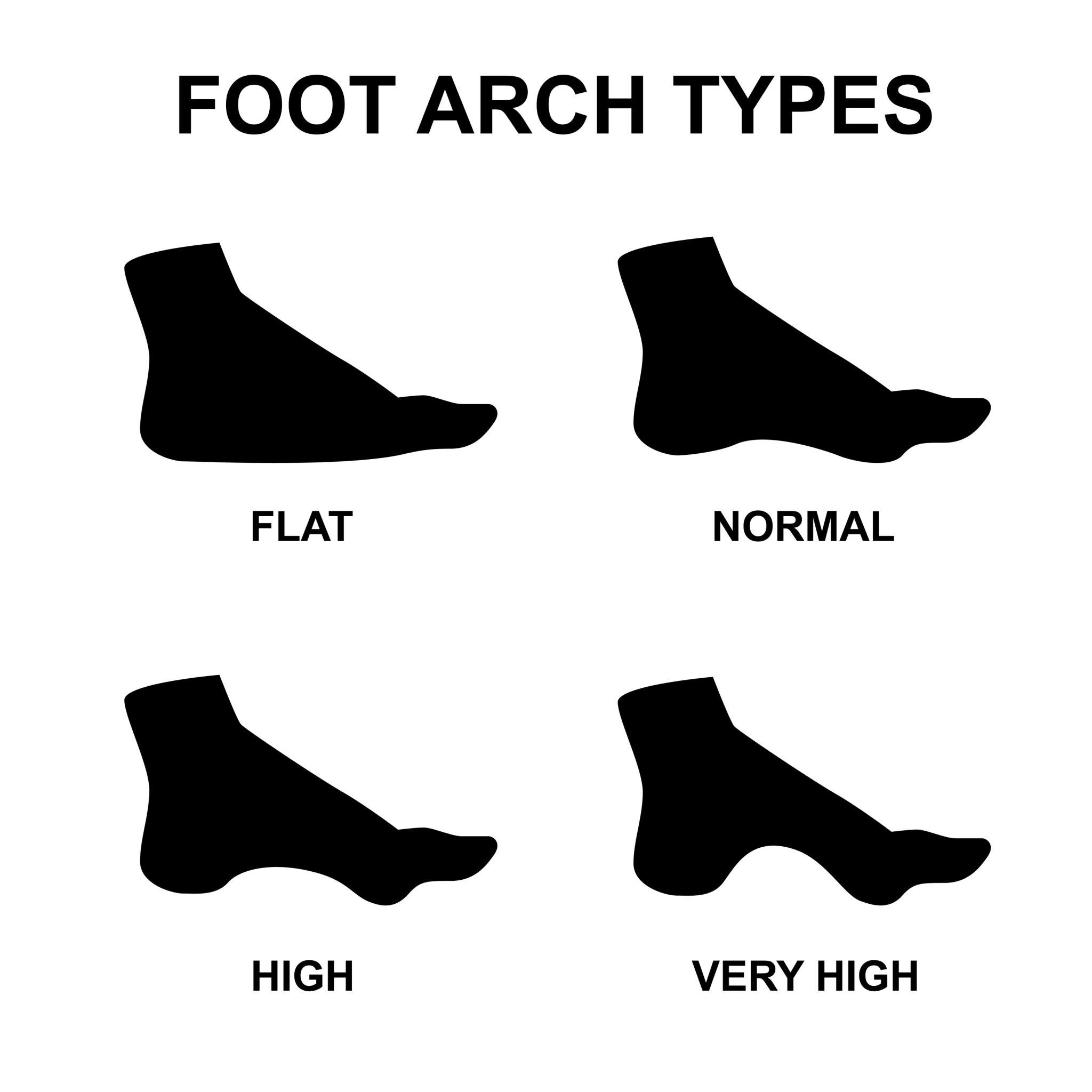
The foot comes in a range of shapes, from the flatter, more pronated pes planus end of the spectrum to the higher-arched, stiffer pes cavus end. In clinic, both get blamed for everything from shin splints to bad vibes. But when it comes to heel pain and Baxter’s nerve, foot shape matters for a more specific reason: it changes how the foot loads, deforms, and transfers force during gait.
And nerves, unlike motivational speakers on Instagram, do not simply “adapt and thrive” when the mechanical environment around them gets rubbish.
First things first: foot posture affects pressure
This much is well supported. A large study by Buldt and colleagues found that foot posture is associated with plantar pressure during gait, and that planus and cavus feet show distinct pressure characteristics. In plain English: different foot shapes do not load the ground in the same way. That matters because heel pain is ultimately a weight-bearing problem, and Baxter’s nerve lives in a part of the heel that is highly influenced by local loading and tissue deformation.
Systematic and experimental work also supports the broader idea that cavus and planus feet distribute pressure differently across the foot. Cavus feet generally show reduced contact area with relatively higher focal loading, while flatter feet often show increased midfoot contact and altered pressure transfer patterns. Again, not shocking—but clinically very important.
Pes planus: the “more contact, more deformation” model
Pes planus is often associated with a lower medial longitudinal arch and a more pronated posture. In one influential case-control study, pronated foot type was associated with chronic plantar heel pain, alongside obesity. That does not prove pronation causes Baxter’s neuropathy, but it does support the idea that a foot posture linked to greater medial loading and tissue deformation may increase local mechanical stress around the heel.
Mechanically, a flatter foot may increase stress in a few ways.
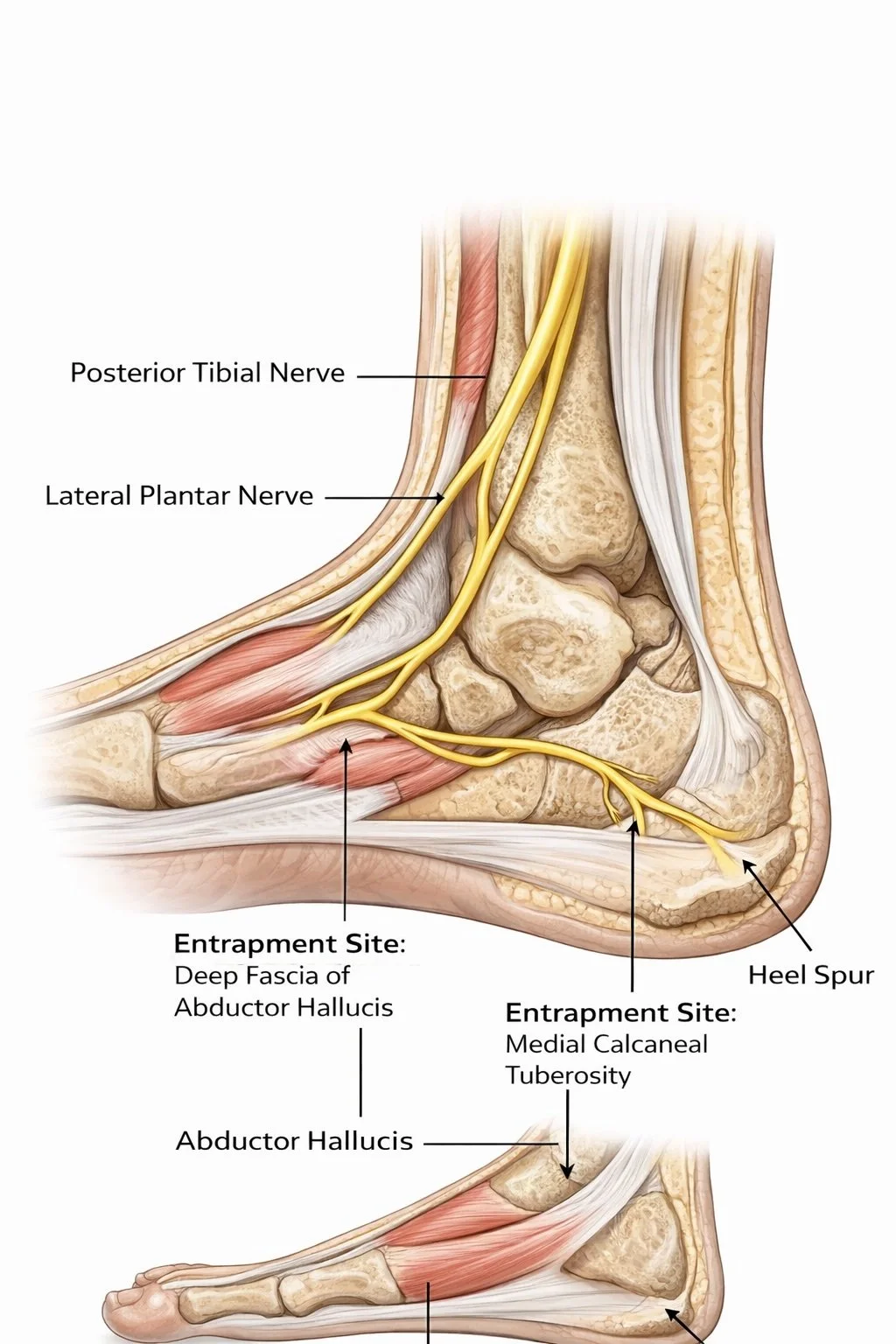
First, the medial structures may experience greater compression and longer contact times as the arch deforms under load. Second, the abductor hallucis region—already implicated as a potential entrapment site for Baxter’s nerve—may be subjected to repeated stretching, thickening, or compression as the foot rolls through stance. Third, if the plantar fascia is chronically overloaded and thickened, this may further reduce space or alter tissue mechanics near the nerve. The anatomy review literature on neural-origin plantar heel pain makes this mechanism plausible, even if direct prospective nerve-stress studies are still lacking.
There is also a pressure-story here.
Flexible flatfoot studies have shown altered plantar pressure patterns during walking and stair tasks, with greater midfoot loading and changes in how force is distributed across the foot. A flatter foot is not just a lower arch in a photograph; it is a different loading strategy in motion. That altered strategy may increase the chance that medial heel soft tissues repeatedly crowd the nerve.
Pes cavus: the “less contact, more focal load” model
Now for the high-arched cousin, pes cavus. Cavus feet are usually stiffer, show reduced contact area, and often concentrate load in smaller regions. Burns and colleagues found that painful pes cavus is associated with distinctive plantar pressure characteristics, helping explain why cavus feet can hurt even when they look impressively “strong” on Instagram. Najafi and colleagues also showed that painful pes cavus alters the distribution of plantar loading during walking.
For Baxter’s nerve, this raises a different mechanical possibility.
Instead of the foot spreading load broadly and deforming more, the cavus foot may create higher local pressures over smaller contact areas, especially under the heel and lateral forefoot. If the rearfoot lands more abruptly or transfers load poorly, the nerve may be irritated by repetitive focal compression near the medial calcaneal region or by compensatory gait strategies elsewhere in the foot. That is a slightly different route to the same bad destination: an annoyed nerve in a crowded neighbourhood.
The key point is that pes cavus does not necessarily protect the heel just because the arch is higher. In fact, reduced shock absorption and more focal loading may increase tissue stress in a different way. So the old “flat foot bad, high arch good” story is biomechanical nonsense dressed up as certainty. Both foot types can create heel pain; they just audition for the role using different scripts.
Pes Planus vs Pes Cavus: How Foot Shape May Alter Nerve Stress and Contribute to Heel Pain
So which foot type is worse for Baxter’s nerve?
Annoyingly, the honest answer is: we do not yet know for sure.
There is stronger direct evidence linking pronated foot posture with plantar heel pain than there is linking cavus feet specifically with Baxter’s neuropathy. But Baxter’s nerve entrapment has multiple proposed contributors, including local anatomy, fascia, muscle bulk, calcaneal spurs, and repetitive loading. So it is entirely plausible that both ends of the posture spectrum can increase nerve stress, just through different mechanical mechanisms.
A reasonable working model looks like this:
Pes planus may increase nerve stress through greater medial deformation, sustained contact, fascial loading, and crowding around the abductor hallucis region.
Pes cavus may increase nerve stress through higher focal pressures, lower shock absorption, and more abrupt or concentrated loading near vulnerable tissues.
That is an inference, not a completed proof. But it fits with what we know about foot posture, plantar pressures, and the anatomy of the nerve.
Static posture is not enough
This is where clinicians can get into trouble. Looking at the foot in standing and declaring, “Ah yes, your arch is the villain,” is a bit lazy. Static posture gives context, but it does not tell you how the foot behaves when walking.
Buldt’s work and related plantar pressure research are useful precisely because they connect foot posture to dynamic loading rather than just visual shape. A foot can look flat and still behave differently depending on stiffness, speed, muscle control, footwear, and pain adaptation. Likewise, a high-arched foot may not be an issue until it becomes rigid, overloaded, and mechanically stingy with shock absorption.
So if you are thinking about Baxter’s nerve, the better question is not merely “Is this foot flat or cavus?” but “How is this foot loading the heel, deforming through stance, and changing the compression environment around the nerve?”
That question is much less sexy for social media. It is also much more useful.
The role of coexisting plantar fascia pathology
One extra complication: plantar fasciitis and Baxter’s neuropathy may coexist. Plantar fascia thickening, calcaneal spurs, and chronic medial heel irritation may all change the local mechanics of the region. So a flatter foot that overloads the fascia may indirectly increase nerve stress, while a cavus foot with focal heel loading may do the same from a different direction. This overlap is one reason heel pain can be such an absolute pest to classify cleanly.
What the research still needs
Here is where future work would be incredibly helpful:
compare confirmed Baxter’s neuropathy cases across pes planus, neutral, and pes cavus groups
map medial heel pressure and pressure-time integrals in those groups
examine whether foot posture changes the strain environment around the abductor hallucis–quadratus plantae interval
explore whether orthoses reduce or increase nerve stress depending on design and foot type
study whether certain foot types are more likely to show mixed fascia-plus-nerve pathology
That last one is particularly important because the current evidence base often lumps all plantar heel pain together, which is a bit like studying “shoulder pain” and hoping the rotator cuff, frozen shoulder, and cervical referral all politely behave the same way. They do not.
Practical takeaway
Foot shape likely alters nerve stress because foot posture changes plantar loading, and plantar loading changes the compression and deformation environment around Baxter’s nerve. A flatter foot may create more medial deformation and tissue crowding. A cavus foot may create more focal loading and less shock absorption. Different mechanics, same possibility: an irritated nerve under a heel that has had enough.
So when someone presents with chronic heel pain, especially if it burns, tingles, or behaves nothing like classic first-step plantar fasciitis, don’t just stare at the arch and guess. Watch the gait. Look at the loading pattern. Think about the nerve.
Because sometimes the arch is not the whole story. Sometimes it is just the scenery while Baxter’s nerve steals the show.
References Buldt AK, Menz HB. Foot posture is associated with plantar pressure during gait: A comparison of normal, planus and cavus feet. Gait & Posture. 2018;62:235-240.
Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure distribution. Journal of Foot and Ankle Research. 2005;48(4):227-234.
Najafi B, Wrobel JS, Burns J. Plantar loading distribution in patients with painful pes cavus. Gait & Posture.2010;32(4):520-525.
Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: A matched case-control study. Journal of Science and Medicine in Sport. 2007;10(5):330-335.
Chundru U, Liebeskind A, Seidelmann F, Fogel J, Franklin P, Beltran J. Plantar fasciitis and calcaneal spur formation are associated with abductor digiti minimi atrophy on MRI of the foot. Skeletal Radiology. 2008;37(6):505-510.
Phillips A, McClinton S. Gait deviations associated with plantar heel pain: A systematic review. Clinical Biomechanics.2017;42:55-64.
Wearing SC, Smeathers JE, Urry SR, Hennig EM, Hills AP. The pathomechanics of plantar fasciitis. Sports Medicine.2006;36(7):585-611.
McPoil TG, Martin RL, Cornwall MW, et al. Heel pain—plantar fasciitis: Clinical practice guidelines linked to the International Classification of Functioning. Journal of Orthopaedic & Sports Physical Therapy. 2008;38(4):A1-A18.
Tedeschi R. Baxter’s nerve: the hidden culprit of chronic heel pain. Neurological Sciences. 2025;46:4685-4689.
Pecina M, Krmpotic-Nemanic J, Markiewitz A. Tunnel Syndromes: Peripheral Nerve Compression Syndromes. CRC Press; 2001.