
The Biomechanics of Medial Heel Loading: How Gait Mechanics May Influence Baxter’s Nerve Compression
Medial heel pain is often shoved into the plantar fasciitis bucket like everything vaguely annoying under the foot. But that’s a bit like calling every loud engine noise “just a car thing.” Sometimes it is plantar fascia. Sometimes it isn’t. And sometimes the real grumpy character is Baxter’s nerve—the first branch of the lateral plantar nerve, also called the inferior calcaneal nerve. It runs through a tight anatomical neighbourhood and can become compressed, irritated, or both. That can produce heel pain that looks suspiciously like plantar fasciitis until you look more closely.
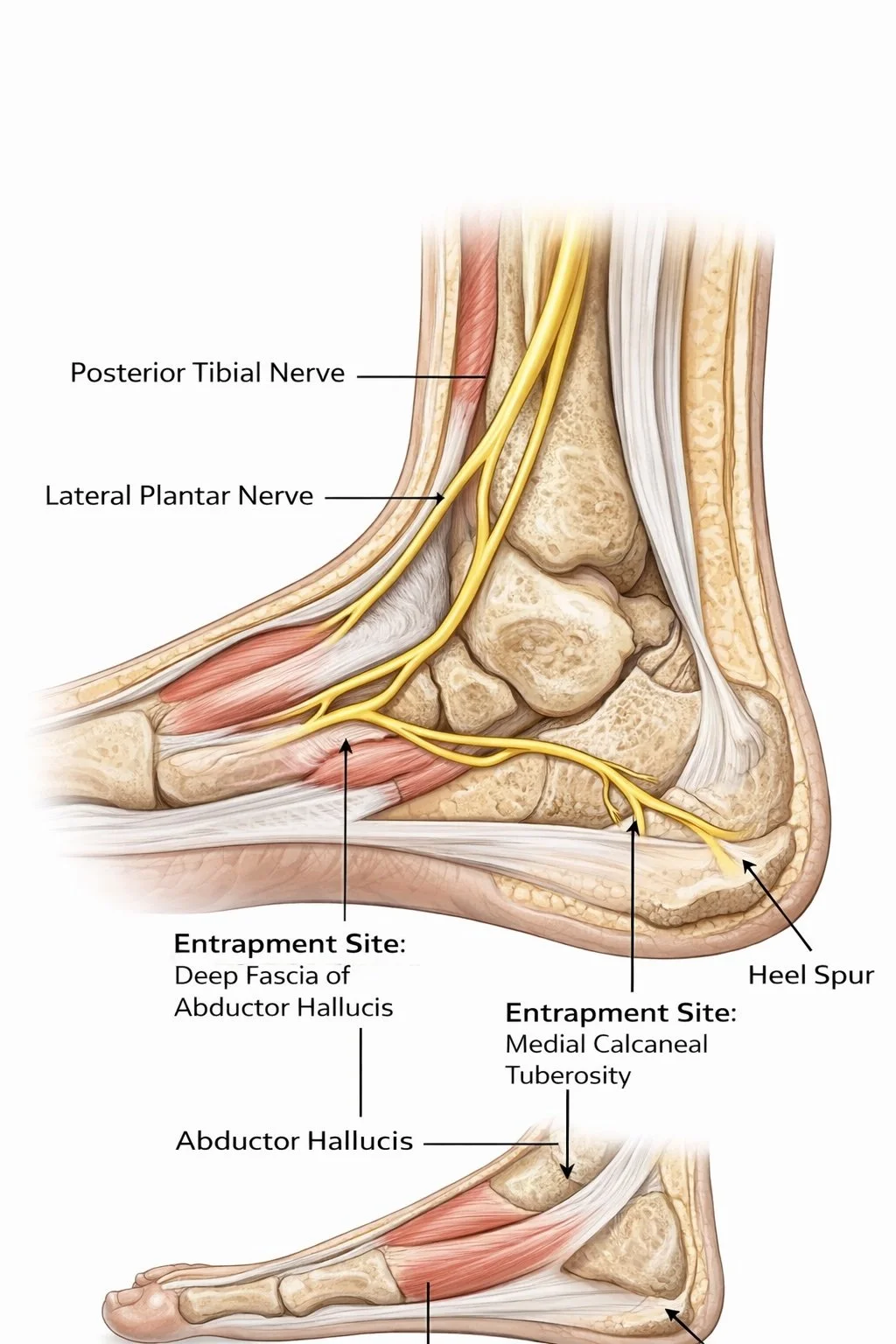
Baxter’s nerve typically courses deep to the abductor hallucis region, then around the medial calcaneal area toward the abductor digiti minimi. That route matters because nerves are not huge fans of being pinched between fascia, muscle, ligament, and bone. In Baxter-related heel pain, two proposed pinch points keep showing up in the literature: one between the deep fascia of abductor hallucis and quadratus plantae, and another near the medial calcaneal tuberosity, where local tissue thickening or bony prominence may add extra compression.
The clinical importance is not trivial. Reviews and case literature repeatedly note that neural causes may account for a meaningful proportion of plantar heel pain, with Baxter’s neuropathy commonly cited as contributing to up to 20% of cases, especially the chronic, treatment-resistant kind. At the same time, a 2025 review made it very clear that some of the imaging assumptions clinicians lean on—especially abductor digiti minimi fatty infiltration as a neat proxy for Baxter’s neuropathy—are not as rock-solid as many people assume. In other words: this is real, relevant, and still a bit diagnostically messy. Welcome to heel pain, where certainty likes to go on holiday.
Why medial heel loading matters
If Baxter’s nerve is vulnerable where it passes around the medial heel, then how load arrives at the medial heel during walking matters. Not in a simplistic “pressure equals pain” way, but in a more useful mechanical sense: gait determines how often, how quickly, and in what direction tissues around the nerve are compressed, stretched, twisted, or forced to adapt.
People with plantar heel pain do not walk identically to pain-free controls. A 2017 systematic review found that gait deviations are present in plantar heel pain, although the exact pattern varies across studies. Meanwhile, plantar pressure work has shown that people with plantar heel pain often alter the way they load the foot during walking, presumably as a protective strategy. Sullivan and colleagues found differences in foot loading during normal walking in people with plantar heel pain compared with controls, suggesting that painful heels are not just sore—they change behaviour.
That finding is important because nerves do not only dislike compression; they also dislike repeated mechanical irritation in a moving system. If gait alters contact timing, rearfoot loading, or medial-lateral pressure transfer, then the soft tissues surrounding Baxter’s nerve may experience a very different mechanical environment step after step after step. That does not prove causation, but it gives us a very plausible framework for why some heels become neuritic rather than merely fascial.
A possible mechanical model: not proven, but very plausible
Here’s the working biomechanical story.
During early stance, the rearfoot accepts load and the foot has to absorb force from above and below, adapt to the ground, and transfer load forward without collapsing into chaos. If the heel strikes into eversion and plantarfelxion, (instead of inverted and dorsiflexed) the rearfoot stays loaded for longer, or if the arch and abductor hallucis region are repeatedly compressed under altered mechanics, then the tissues, most likely the skin, around the inferior calcaneal nerve may be exposed to chronic irritation. Add local fascial thickening, calcaneal spur formation, or muscle bulk, and the nerve may have even less room to behave itself.
This becomes even more interesting when you look at plantar heel pain research more broadly. Chronic plantar heel pain has been associated with pronated foot posture in some work ( and I see in my clinic and pressure plate finding), particularly the classic matched case-control study by Irving and colleagues. That does not mean every pronated foot becomes painful, but it does suggest that a foot posture which increases medial loading or changes how tissues deform over time may increase strain on the local system.
Now, to be fair, later work has not always shown dramatic differences in simple clinical foot posture measures between people with and without plantar heel pain. So this is not a story where one static measure wins the trophy. Static posture is not gait, and gait is not a single pressure number. The more honest interpretation is that dynamic loading patterns likely matter more than one frozen snapshot of the foot in standing.
Medial heel loading is not just about “too much pronation”
This is where the internet usually goes off the rails. Someone says “medial heel pain,” someone else yells “overpronation,” and suddenly the whole conversation gets reduced to a cartoon. Real gait is messier than that.
Medial heel loading depends on several interacting factors:
rearfoot position at contact
subtalar motion and timing
tibial rotation
arch deformation
big toe function later in stance
walking speed and step strategy
pain-related compensation
Each of these can shift where plantar pressure goes and how soft tissue tension develops. The Baxter nerve sits in a region influenced not just by the plantar fascia, but by the abductor hallucis fascia, quadratus plantae, long plantar ligament, calcaneal periosteum, and local muscle bulk. So the nerve can be irritated by a whole neighbourhood problem, not just one naughty structure acting alone.
What do imaging studies add?
MRI has been useful, but with a few caveats. One of the classic clues linked to Baxter’s neuropathy is fatty atrophy or infiltration of the abductor digiti minimi muscle, which may indicate denervation. Older MRI studies helped popularise this idea, and more recent papers still discuss it. But the newer review evidence says the association remains uncertain because the overall evidence base is still not robust enough to treat this sign as a slam-dunk diagnostic marker in isolation. So MRI can help, but it should not be treated like a magical truth oracle descending from radiology heaven.
Where gait analysis becomes clinically useful
If a patient has medial heel pain that behaves like plantar fasciitis on paper but does not respond like plantar fasciitis in real life, gait deserves a closer look.
Questions worth asking include:
Is the rearfoot loading asymmetrically?
Is there prolonged or repeated compression through the medial heel?
Does pain increase as walking accumulates, suggesting repeated irritation rather than just “first-step” fascial pain?
Are there neurological features such as burning, tingling, or altered sensation?
Is the person offloading one part of the foot and overloading another?
This matters because the classic symptom pattern differs. Plantar fasciitis is famous for first-step pain. Baxter’s neuropathy more often worsens with activity and may include burning, paresthesia, or radiation. Those differences are not absolute, but they are very clinically useful.
What the research still needs
This is the juicy bit for clinicians and researchers.
The literature strongly suggests Baxter’s nerve entrapment is real and under-recognised, but direct biomechanical evidence remains thin. We still need better work on:
medial heel pressure patterns in confirmed Baxter’s neuropathy
whether prolonged medial rearfoot loading predicts neural symptoms
how abductor hallucis and quadratus plantae thickness relate to nerve irritation
whether certain gait strategies increase compression at the two proposed entrapment sites
which movement-based treatments actually reduce neural irritation, not just pain scores
At the moment, we are making a reasonable biomechanical inference from anatomy, symptom behaviour, plantar pressure research, and plantar heel pain gait studies. That is useful, but it is not the same as having a beautifully designed prospective study that says, “Yes, this exact loading pattern squashes the nerve like a grumpy sandwich.” Science has not fully handed us that gift yet.
The practical takeaway
The biomechanics of medial heel loading likely matter because gait determines the compression environment around Baxter’s nerve. In people with persistent medial heel pain, especially when symptoms worsen with activity or include burning and tingling, looking only at the plantar fascia may miss the plot entirely. Baxter’s nerve sits in a mechanically busy part of the foot, and abnormal loading patterns may influence whether that nerve stays quiet or starts shouting.
So yes, plantar fasciitis is common. But it should not be allowed to become the heel pain version of “Have you tried turning it off and on again?”
Research ReferencesTedeschi R, et al. Baxter’s nerve: the hidden culprit of chronic heel pain.Foot and Ankle Clinics. 2025.
Allam AE. Plantar Heel Pain.StatPearls Publishing. 2024.
Pecina M, Markiewitz A, Krmpotic-Nemanic J. Tunnel Syndromes: Peripheral Nerve Compression Syndromes.CRC Press; 2001.
Jaring MRF, et al. Bilateral Baxter’s neuropathy secondary to nerve impingement.Foot & Ankle Specialist.2019.
Chundru U, Liebeskind A, Seidelmann F, et al. Plantar fasciitis and calcaneal spur formation associated with abductor digiti minimi atrophy on MRI.Skeletal Radiology. 2008.
Phillips A, McClinton S. Gait deviations associated with plantar heel pain: a systematic review.Clinical Biomechanics. 2017;42:55-64.
Sullivan J, et al. Plantar heel pain and foot loading during normal walking.Gait & Posture. 2015.
Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a case-control study.Journal of Science and Medicine in Sport. 2007.
McPoil TG, Martin RL, Cornwall MW, et al. Heel pain—plantar fasciitis: clinical practice guidelines.Journal of Orthopaedic & Sports Physical Therapy. 2008.
Coles IR, et al. Ultrasound block of the first branch of the lateral plantar nerve for chronic heel pain.Pain Physician. 2021.
Choudhary S, et al. Baxter’s nerve entrapment: the missing nerve in plantar heel pain.Archives of Medicine and Health Sciences. 2024.
Presley J, et al. Chronic heel pain due to entrapment of the inferior calcaneal nerve.Foot & Ankle International. 2013.
Irving DB, Cook JL, Young MA, Menz HB. Obesity and pronated foot posture as risk factors for plantar heel pain.Medicine & Science in Sports & Exercise. 2007.