
How Talus Misalignment Can Lead to Bunions: A Manual Therapist’s Guide
For attendees of the Feet Mechanics Workshop
By Riccardo Galeotti | The Body Lab | 8 May 2025
Why does talus misalignment matter in bunion formation?

Bunions (hallux valgus) are more than a cosmetic deformity—they’re a biomechanical consequence of whole-foot dysfunction. While genetics, tight footwear, and joint hypermobility are often blamed, a deeper structural issue—talus misalignment—frequently plays a central role.
The talus serves as the keystone of the ankle-foot complex, transferring load between the leg and the foot, guiding pronation/supination transitions, and influencing medial arch function. If it becomes misaligned due to injury, habitual gait compensations, or poor foot control, the body’s centre of mass shifts medially, destabilising the first ray. This sets up the foot for progressive structural failure, including:
First metatarsal drifting medially
Hallux abducting laterally
Increased strain on the medial capsule and sesamoids
As discussed in the Feet Mechanics Workshop and your bunion webinar, this shift begins long before visual signs of bunion appear. You can also watch how to assess the Talus function here
“An unstable or misaligned talus results in altered medial column loading, contributing significantly to hallux valgus formation” (McPoil et al., 2009¹).
How does talus misalignment create bunions biomechanically?
Foot mechanics are a chain reaction. Misalignment of the talus causes:
Prolonged pronation: The foot remains unlocked for too long during midstance.
Delayed supination: Without re-supination, the medial arch cannot lift or load effectively for toe-off.
First ray instability: The metatarsal lacks a stable base, causing the big toe to deviate laterally.
Abductor hallucis inhibition: This intrinsic muscle can’t counteract valgus force due to positional disadvantage.
Second toe collapse: Often seen as forefoot instability spreads, shifting more weight medially.
This is reinforced by footwear with narrow toe boxes, which restrict toe splay, dorsiflexion, and natural load sharing between digits. MRI studies confirm that talar positioning influences forefoot abduction torque and sesamoid tracking (Lee et al., 2013³; Kim et al., 2015⁷).
“The subtalar joint’s prolonged eversion and delayed heel rise increase stress on the first ray” (Smith & Katchis, 2013⁶).
When should you suspect talus misalignment in clinical practice?
Red flags for talus dysfunction include:
Flat feet or collapsed arches that don’t reappear during supination
Limited ankle dorsiflexion, particularly with eversion
Early heel rise or excessive medial forefoot loading in gait
Callus under 1st or 2nd metatarsals, indicating overload
Sesamoid pain or tenderness at the medial hallux joint
History of ankle sprains, hypermobility, or altered gait
Functional assessments (such as foot tripod tests, single-leg stance, or heel raise assessments) often show the first ray fails to anchor properly or collapses under load. In gait, watch for insufficient toe dorsiflexion during push-off, or a first toe that rotates outward instead of pushing straight ahead.
These signs suggest the talus is failing to guide the subtalar and midfoot joints efficiently, leading to bunion-prone mechanics.
What does this mean for treatment—and what should we do about it?
Treating bunions without addressing talus mechanics is incomplete. Toe spacers, surgery, and orthotics may address symptoms, but long-term success depends on restoring proximal control and joint timing.
Manual therapists should:
Mobilise the talus posteriorly and medially to restore joint glide
Address midfoot mobility (navicular, cuboid, cuneiforms) to re-establish foot tripod
Use functional drills to train pronation-supination sequencing during gait
Activate intrinsic foot muscles (e.g. abductor hallucis) and retrain toe splay
Implement hip and pelvic stability exercises to prevent compensation from above
For clients, understanding that bunions develop over time and can be reversed—or at least slowed—without invasive measures is empowering.
“Mobilisation of the talus and midfoot improves rearfoot alignment and first ray stability” (Vicenzino et al., 2008⁵).
Learn this and more in the Feet Mechanics Workshop
This topic is just the beginning. The Feet Mechanics Workshop covers how the foot moves in all three planes, how dysfunction propagates through the body, and how to use movement, manual therapy, and education to get long-lasting results.
ReferencesMcPoil TG, Cornwall MW. Relationship between foot function and the development of hallux valgus. J Foot Ankle Res. 2009;2(1):11.Dakin SG, Newton J, Martinez FO, et al. Chronic inflammation is a feature of Achilles tendinopathy and rupture. Br J Sports Med. 2018;52(6):359–67.Lee JH, Lee HS, Kim JS, et al. Relationship between first ray hypermobility and the severity of hallux valgus deformity. J Orthop Surg (Hong Kong). 2013;21(2):199–202.Nigg BM, Benno M. The role of joint motion in foot function and pathology. Clin Biomech. 2011;26(5):452–460.Vicenzino B, Branjerdporn M, Teys P, Jordan K. Initial changes in posterior talar glide and pain after mobilization with movement in patients with ankle sprain. Man Ther. 2008;13(5):492–500.Smith RW, Katchis SD. Foot biomechanics and hallux valgus. Orthop Clin North Am. 2013;44(4):405–14.Kim Y, Kim JS, Young KW, Naraghi AM. Radiographic measurements of the first metatarsophalangeal joint in hallux valgus. Foot Ankle Int. 2015;36(3):366–372.
Ehlers-Danlos Syndrome (EDS) is often misunderstood as simply being “double-jointed” or unusually flexible. In reality, EDS is a complex connective tissue disorder that affects joint stability, proprioception, pain processing, fatigue, autonomic function, and movement control throughout the entire body.
For therapists, this creates a unique clinical challenge. Many traditional rehabilitation approaches that work well for the general population—including aggressive stretching, heavy manual therapy, or isolated strengthening—can sometimes worsen symptoms in people with EDS. What appears to be weakness may actually be instability. What appears to be tightness may be a protective strategy. And what appears to be a local joint problem may reflect a much larger whole-body compensation pattern. Understanding EDS requires a shift away from simply chasing pain or increasing mobility and towards improving control, body awareness, load management, nervous system regulation, and long-term resilience.
In this article, we explore the current evidence surrounding EDS, including proprioception, pain, strength training, autonomic dysfunction, fascia, breathing mechanics, and the role of whole-body assessment. We also examine where emerging concepts such as biotensegrity and fascial therapy may fit within modern clinical practice and discuss the key principles every therapist should understand when working with hypermobile patients.
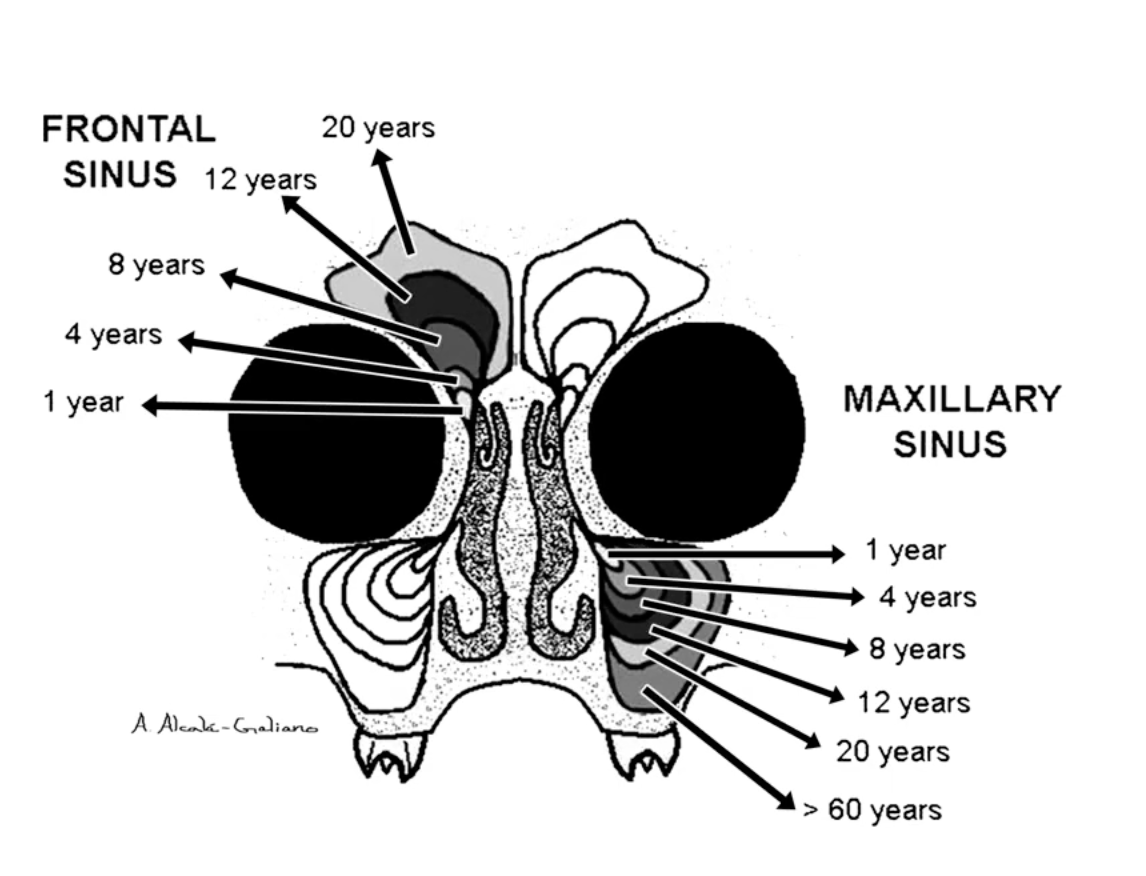
Most people think cavities are caused by sugar alone. But the way you breathe may be playing a bigger role than you realise. Nasal breathing supports saliva production, healthy sinus development and proper facial growth, while chronic mouth breathing has been linked to dental crowding, dry mouth and an increased risk of tooth decay. Discover why your nose may be one of the most important tools for protecting your teeth and shaping your face.

Most people assume breathing exercises and breathing retraining are the same thing.
They’re not.
In fact, this misunderstanding may be one of the biggest reasons people continue to struggle with poor sleep, jaw tension, anxiety, headaches, fatigue, and breathing-related problems despite regularly practising breathing techniques.
Think about it.
The average person takes around 20,000 breaths every day.
A five-minute breathing exercise might influence a few dozen of them.
What about the other 19,900?
This is where breathing retraining becomes different. Rather than focusing on a specific exercise, breathing retraining aims to change your everyday breathing patterns—while you’re working, walking, talking, sleeping, exercising, and dealing with stress.
In this article, we’ll explore why breathing exercises alone often fail to create lasting change, the difference between breathwork and breathing retraining, and how improving your default breathing habits may have a greater impact on your health than any breathing technique.
Most of us never think about breathing until something goes wrong.
A blocked nose. Poor sleep. Anxiety. Headaches. Jaw tension. Fatigue.
The common assumption is that we need more oxygen. But what if the problem isn’t a lack of oxygen at all?
Modern research suggests that many people breathe far more than their bodies actually require. In doing so, they may be disrupting the delicate balance between oxygen and carbon dioxide that helps regulate blood flow, nervous system function, sleep quality and even oxygen delivery to the tissues.
In this article, we’ll explore why bigger breaths aren’t always better, why carbon dioxide may be one of the most misunderstood gases in human physiology, and how your breathing habits could be influencing everything from jaw tension and posture to energy levels and recovery.

When most people develop jaw pain, clicking, clenching, or teeth grinding, attention immediately turns to the jaw joint itself.
Makes sense.
After all, that’s where the symptoms are.
But what if the jaw isn’t actually the starting point?
What if it’s simply the place where a much larger story is being expressed?
Emerging research suggests that many cases of TMJ dysfunction may involve far more than joint mechanics alone. Breathing patterns, sleep quality, nervous system regulation, tongue posture, neck tension, stress, and even the way the brain processes sensory information may all play important roles.
In other words, your jaw might not be malfunctioning because it is broken.
It might be working overtime because other systems are struggling.
In this article, we’ll explore the fascinating relationship between the jaw, neck, airway and nervous system—and why treating the jaw alone may not always provide lasting relief.

Most people think stress lives in the mind. Others think it lives in the shoulders. But what if one of the body’s favourite places to store stress is your jaw?
Emerging research suggests the jaw is connected to emotional processing, pain perception, breathing, posture and even activity within the brain’s limbic system. Learn how jaw tension, chronic stress and inflammation may be influencing headaches, neck pain, fatigue and persistent pain—and why treating the whole person matters more than chasing symptoms.

At a kids’ sporting match over the weekend, I watched a gentleman walking in thongs and immediately noticed something I see constantly in clinic: his body barely changed shape from heel strike through to mid-stance. His ankle stayed stiff, his knee barely adapted, and his pelvis remained locked in one position. Over time, this type of walking pattern can reduce force absorption, overload the lumbar spine, affect circulation, compress nerves, and contribute to chronic pain. Here’s why walking is really a force-management system — and what happens when the body loses its ability to adapt.
Most people think protein speeds up every type of tissue repair equally. New research says otherwise. Muscle rebuilds relatively quickly, but tendons, cartilage, ligaments, and bone operate on dramatically slower timelines — sometimes taking years to fully remodel. Here’s what that means for recovery, rehab, ageing, and why your tendon couldn’t care less about your two-week protein challenge.
Think posture is about sitting up straight? Think again. Posture isn’t a position—it’s a reflection of what your body can feel, move, and control. In this article, we break down what posture really is, why your nervous system is calling the shots, and how movement—not stiffness—is the key to changing it.
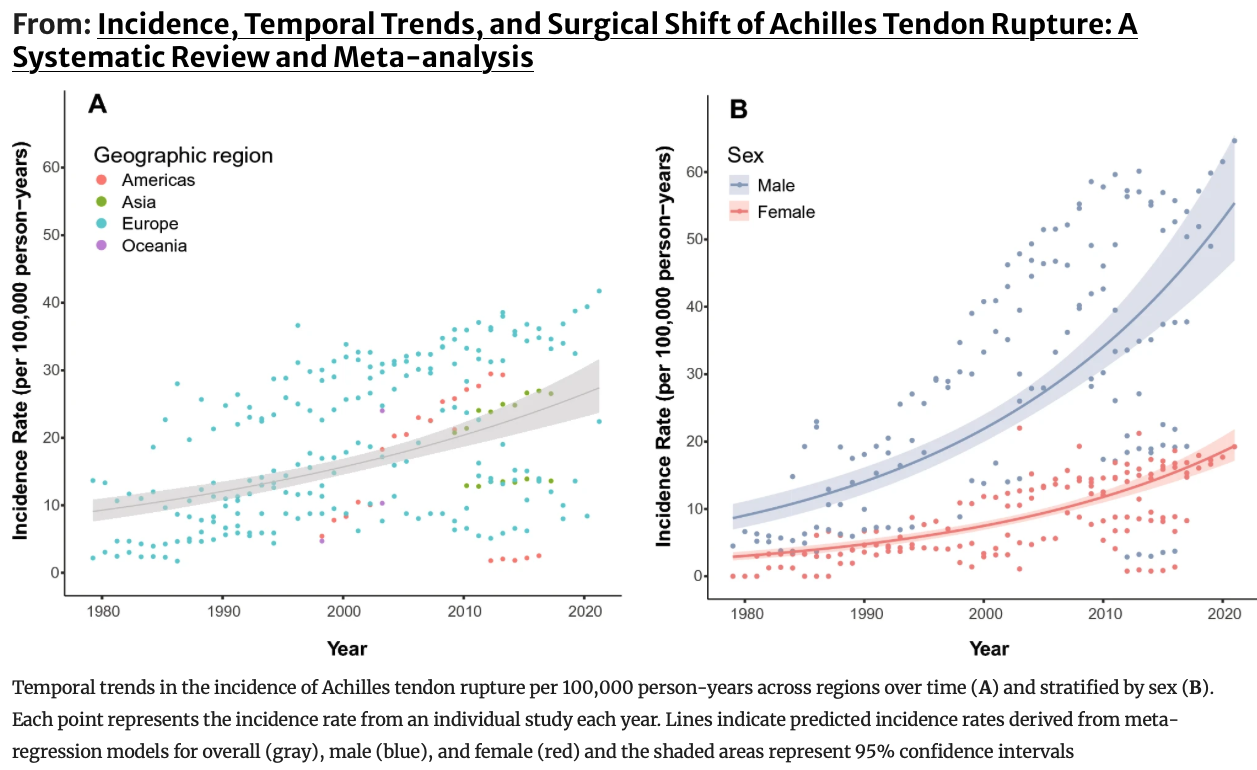
Achilles tendon ruptures are increasing worldwide. Learn why it’s happening, what the latest research shows, and how to improve tendon strength, foot mechanics, and prevent injury.

Struggling with bone loss or worried about osteoporosis? Learn how strength training, impact exercise, and balance work can improve bone health. Insights from Canberra physios at Next Gen.

Discover how foot pressure plate analysis in Canberra reveals how you walk, move, and load your body. Advanced gait assessment at The Body Lab.

A 2025 study suggests stimulating lymphatic vessels in the neck can double brain waste clearance—but before you start massaging your face non-stop, let’s break down what the research actually shows. From sleep and movement to fluid dynamics, this guide explains how your body really supports brain health—and where therapy fits in.

Cluster headaches are severe, recurring, and often resistant to medication. This guide explores how acupuncture and cranial therapy in Canberra can help reduce pain, frequency, and improve long-term outcomes.

Poor sleep affects hormones, metabolism, pain, and recovery. Evidence-based insights with Australian sleep data and metabolic perspective.

Persistent pain is not always caused by tight muscles or stiff joints. In many cases the nervous system and skin play a key role. Understanding this connection can change how chronic pain is treated.
Dermo-Neuro Modulating is a gentle manual therapy technique that works through the skin to calm irritated nerves and reduce pain. Developed by physiotherapist Diane Jacobs, it offers a modern, neuroscience-informed approach to treating persistent pain conditions.

Ankle sprains are often treated as ligament injuries, but the mechanics of the foot tell a much bigger story. One structure that frequently goes unnoticed is the Flexor Hallucis Longus (FHL) — the tendon that connects the calf to the big toe and plays a critical role in propulsion, arch stability, and walking efficiency. Because this tendon runs through a narrow tunnel behind the ankle joint, it can be compressed or irritated during common inversion ankle sprains. Understanding how the FHL contributes to foot mechanics may help explain persistent ankle stiffness, reduced push-off power, and ongoing pain after injury. Exploring the role of the big toe in ankle recovery offers a more complete view of foot biomechanics and movement rehabilitation.

If you’ve ever searched “acupuncture for pain Canberra”, chances are something in your body has decided it’s had enough. Maybe it’s your heel barking every morning, a shoulder that refuses to behave, or a lower back that stiffens the moment you sit down too long.
Acupuncture can be remarkably effective for reducing pain. But here’s the honest truth most clinics won’t say out loud:
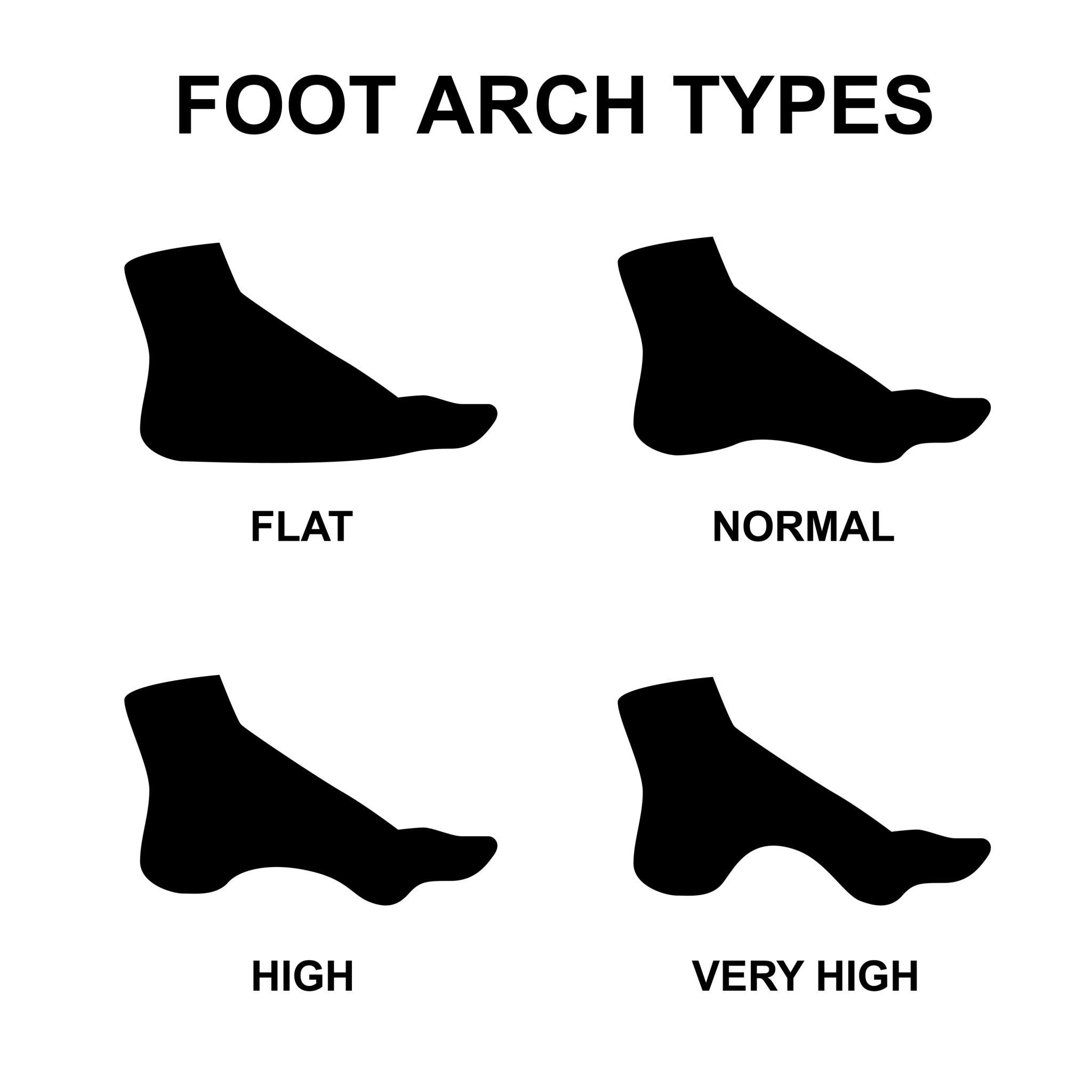
Foot shape plays an important role in how the foot absorbs force and distributes pressure during walking. From flatter pes planus feet to the higher-arched pes cavus foot type, these structural differences influence how load travels through the heel and arch.
Understanding how these loading patterns affect the tissues around the heel—including the plantar fascia and Baxter’s nerve—may help explain why some people develop persistent heel pain while others do not.
Most cases of heel pain are quickly labelled plantar fasciitis, but that diagnosis doesn’t always tell the full story.
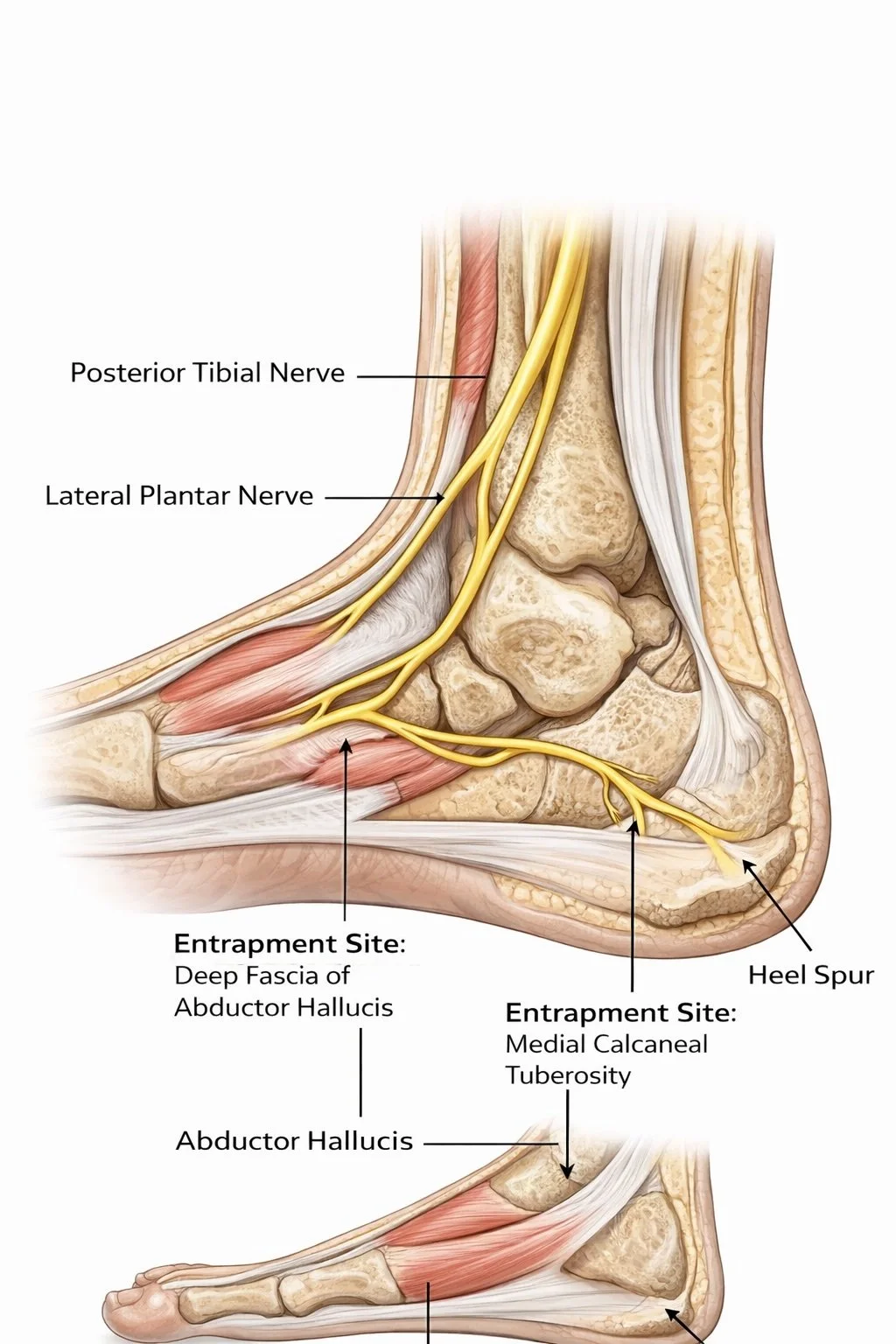
Research suggests that Baxter’s nerve entrapment—compression of the inferior calcaneal nerve—may account for up to 20% of chronic heel pain cases. Because the symptoms overlap with plantar fasciitis, this nerve condition is frequently overlooked.
Understanding how gait mechanics and medial heel loading influence the tissues surrounding Baxter’s nerve can help explain why some heel pain persists despite traditional treatments.
Most cases of heel pain are quickly labelled plantar fasciitis, but that diagnosis doesn’t always tell the full story.In fact, research suggests that up to 20% of chronic heel pain cases may involve compression of Baxter’s nerve, a small branch of the lateral plantar nerve that runs along the inside of the heel. Because the symptoms overlap, Baxter’s nerve entrapment is frequently mistaken for plantar fasciitis.While plantar fasciitis involves irritation of the plantar fascia, Baxter’s neuropathy is a nerve compression problem, which means the symptoms, mechanics and treatment considerations can be quite different.
Understanding the difference is important. Treatments designed for plantar fascia inflammation may not help nerve-related heel pain—and in some cases may even aggravate the underlying problem.
In this article we explore the key anatomical and biomechanical differences between these two conditions and explain why a deeper look at foot mechanics and gait can be crucial when heel pain persists.

Heel pain when walking is one of the most common problems I see at The Body Lab in Canberra. Here’s why it happens and how improving foot mechanics can help.
Foot pain is often treated locally, but the real cause may lie in how your foot and ankle manage force during movement. Learn how foot mechanics, tendon loading and gait influence heel pain, plantar fasciitis, posture and movement efficiency.

Most people think stress is all adrenaline and action.
But there’s another version — the quiet one. The one where motivation fades, energy drops, and your nervous system stops fighting and starts conserving.
This isn’t weakness. It’s biology.
Research from Martin Seligman and earlier work by Curt Richter showed that when stress becomes uncontrollable, the brain shifts into a shutdown pattern known as learned helplessness.
At a chemical level, this state is linked to altered acetylcholine signaling, increased nitric oxide, reduced thyroid hormone activity, and impaired mitochondrial energy production. In simple terms? Your metabolism and your mood are having the same conversation.
The good news: the nervous system is plastic. Environment, light exposure, movement, social connection, and metabolic support all influence whether the brain adapts toward resilience — or surrender.
Helplessness isn’t a character flaw.
It’s a reversible physiological state.

Tendon pain doesn’t heal with rest alone. Modern research shows tendons need the right kind of load, at the right time, to recover. This article breaks down what actually works — using the latest evidence from leading tendon researchers — and explains why rehab advice often sounds confusing but isn’t wrong.

I think people are expecting to be fixed in one session and people don’t realise the amount of joints and muscle connections in the lower body and the work needed (strength) and connectiveness (joint sequencing) to actually have a foot or lower limb function in walking.
The lower limb is not a single joint or muscle problem. It is a highly complex, multi-joint system that relies on precise timing, coordination, and load sharing between joints, muscles, tendons, ligaments, and the nervous system (Neumann, 2017; Standring, 2021).
Many people expect foot or knee pain to be “fixed” in one session.
But walking is a whole-body task involving nearly 78 joints, the nervous system, and connective tissue that adapts slowly over time. This article explains why real change takes longer — and why that’s exactly how lasting results happen.
Riccardo Galeotti doesn’t treat pain by chasing symptoms — he looks at how your body actually moves. As the founder of The Body Lab Canberra, Riccardo combines biomechanics, gait analysis, movement therapy, and acupuncture to uncover the patterns driving recurring pain. By focusing on how you walk, load, and adapt to gravity, his work helps clients move better, feel stronger, and build long-term resilience — not just short-term relief.