Understanding the Windlass Mechanism: Why Your Plantar Fascia Deserves More Credit
Let’s talk about that stringy bit in your foot that holds your entire walking life together—the plantar fascia. It’s the unsung hero of movement, and its starring role? The Windlass Mechanism.
If you’re a manual therapist, myotherapist, or just foot-curious, buckle up (or lace up). This mechanism isn’t just academic trivia—it’s biomechanical gold for assessment, rehab, and treating persistent heel pain.
What Is the Windlass Mechanism, Really?
The Windlass Mechanism describes the biomechanical process where the plantar fascia tightens as the toes dorsiflex (bend upwards), especially during the toe-off phase of gait. The word “windlass” comes from a medieval pulley system, because—stay with me here—the plantar fascia works like a winch.
Here’s the magic:
As the toes lift, the fascia winds around the metatarsophalangeal joints, pulling the calcaneus (heel bone) closer to the metatarsal heads, lifting the arch like a drawbridge mid-step. This action stiffens the foot, turning it from a squishy shock-absorber into a powerful lever ready for propulsion.
The Three Types of Windlass: Passive, Reverse, and Active
To truly appreciate this mechanism, we need to differentiate its three operational modes:
1. Passive Windlass
This is the classic model most of us learned: during toe dorsiflexion (especially the big toe), tension builds in the plantar fascia without muscular input. This tightens the fascia and elevates the arch. Think of it as the foot’s natural mechanical gear-shift for propulsion. Hicks (1954) was the first to observe that this mechanism functions even in cadavers, confirming it’s primarily a passive, not muscular, action.
2. Reverse Windlass
This occurs during the early stance phase (heel strike through mid-stance), where elongation of the arch and flattening of the foot stretches the plantar fascia. This eccentric lengthening stores elastic energy in the fascia, priming it for recoil later in the step. It's a key part of foot pronation mechanics.
3. Active Windlass
Muscles aren’t just bystanders. Intrinsic foot muscles like the flexor hallucis brevis and extrinsic players like the flexor hallucis longus actively contribute to maintaining the arch and aiding toe-off. The active windlass becomes critical when passive structures are insufficient or overburdened—such as in chronic cases of plantar fasciitis or with flatfoot deformities.
The Role in Gait: From Marshmallow to Lever
During the stance phase of walking, the foot must be flexible enough to absorb shock and conform to the ground. But just before take-off, it needs to transform—literally—into a rigid lever to launch you forward.
Cue the windlass:
Toes dorsiflex
Plantar fascia tightens
Arch rises and stabilises
Force transfers efficiently up the kinetic chain
It’s like switching from a beanbag to a springboard—except it happens every single step without conscious thought.
When the Windlass Fails: Fascia Freakouts & Foot Pain
Now for the dark side. When the windlass mechanism is dysfunctional—due to restricted toe extension, midfoot stiffness, or a tight fascia—it stops performing its “tighten and lift” routine. That’s when things get messy.
Common consequences?
Plantar fasciitis: Chronic overload causes inflammation and microtears
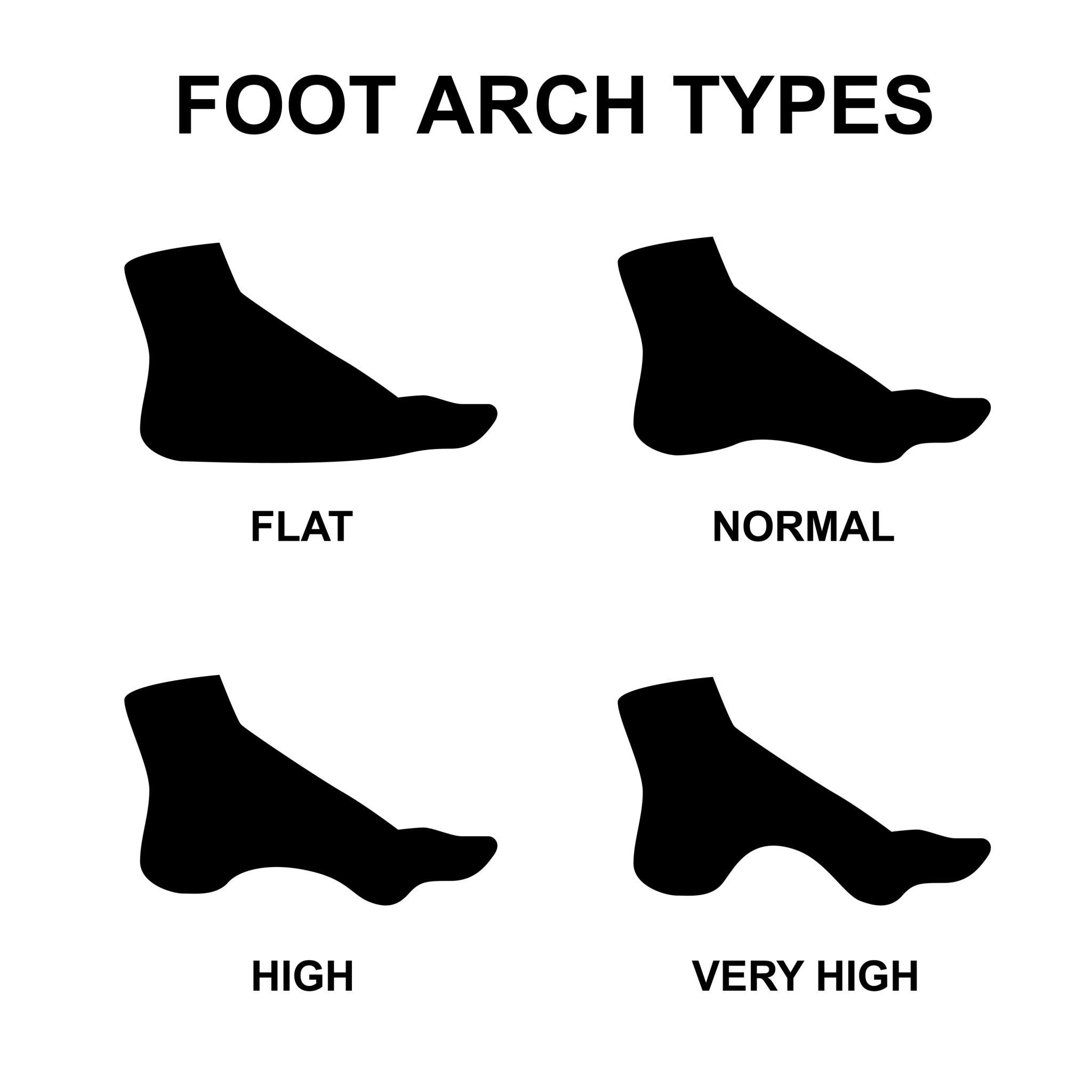
Flat feet: Lack of arch lift leads to pronation chaos
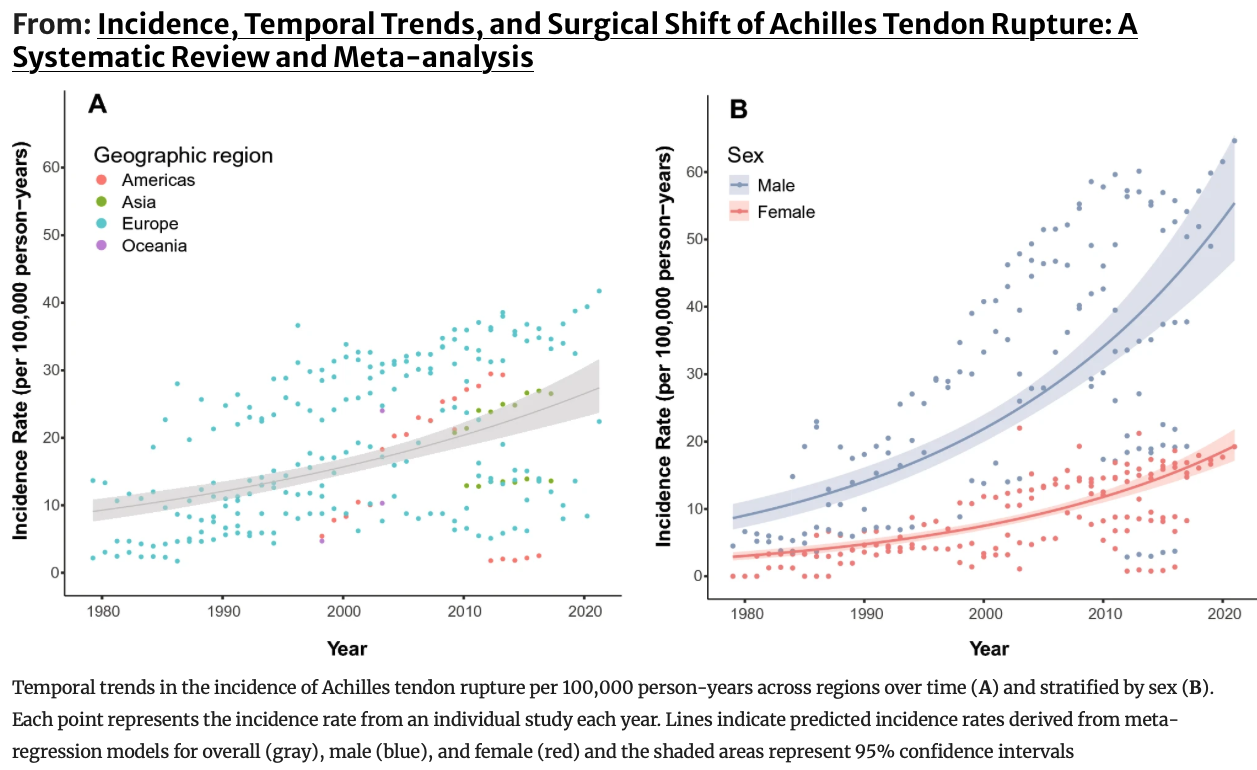
Achilles strain: Poor energy transfer makes the calf do all the work
Knee or hip overload: Poor foot mechanics ripple upstream
According to Okamura et al. (2020), individuals with plantar heel pain often show reduced windlass function, altered toe dorsiflexion, and compensated push-off mechanics—which only worsens the problem if not addressed.
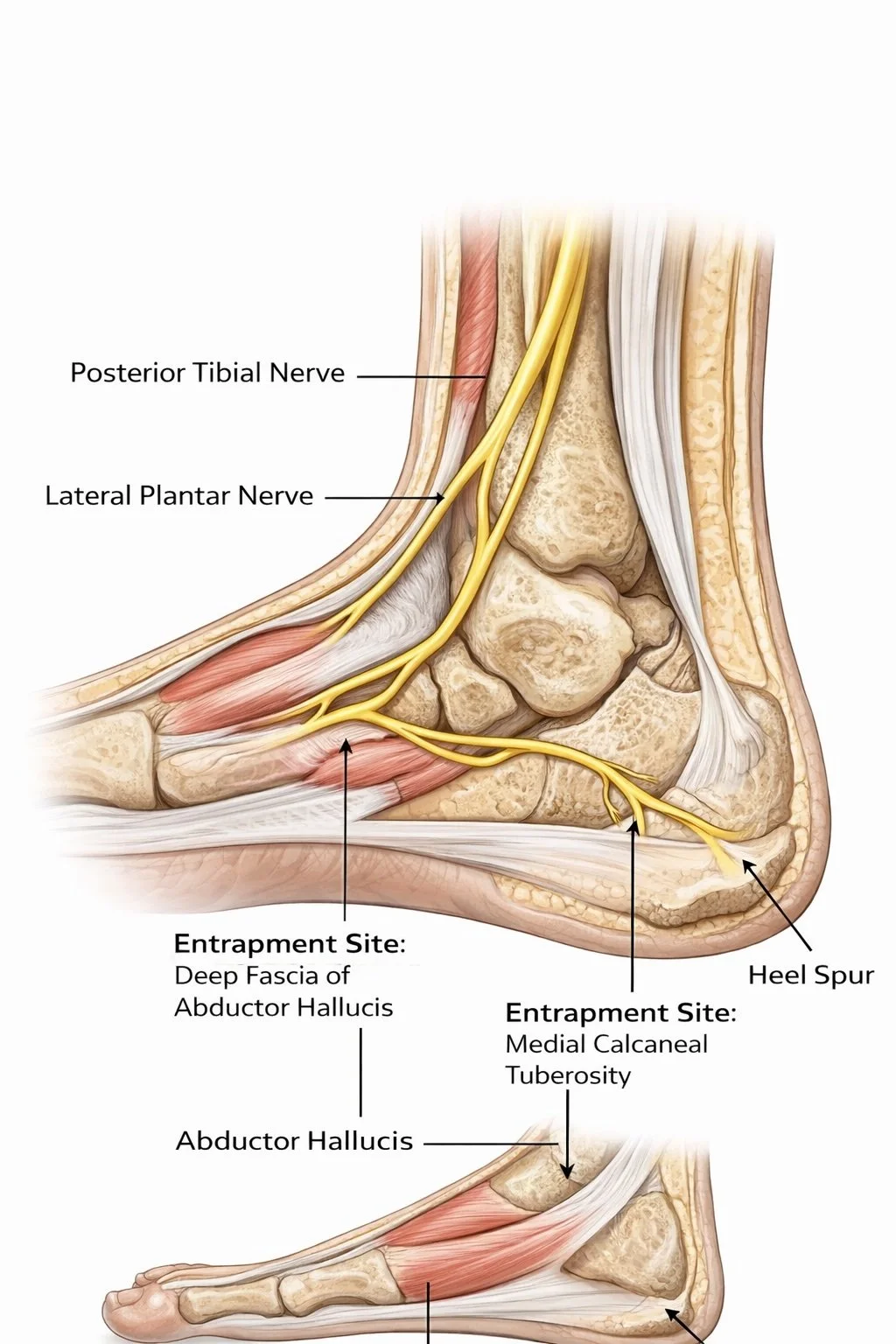
Anatomy 101: The Great Toe and Arch Control
Back in 1954, J.H. Hicks laid the groundwork. In his seminal study on cadavers and live subjects, Hicks observed that as the great toe extends:
The medial longitudinal arch height increases
The calcaneus inverts
The tibia externally rotates
The plantar fascia tightens visibly like a band
He concluded this wasn’t primarily driven by muscles—this was an anatomical design feature. A beautifully efficient one.
Caravaggio et al. (2009) further confirmed the plantar aponeurosis connects the heel to the toes, with the strongest load bearing occurring beneath the first metatarsophalangeal joint (MTPJ). As you toe off, the arch lifts in response to this tension. Efficient. Effective. Elegant.
Gait Phases and the Windlass
Initial Contact: Plantar fascia begins lengthening under load (reverse windlass in action)
Loading Response to Mid-Stance: The arch lowers, absorbing shock. Muscles work eccentrically.
Terminal Stance to Toe-Off: Great toe dorsiflexes, fascia tightens, arch lifts (passive and active windlass co-activate)
During push-off, approximately 45–55 degrees of great toe extension is required (Neumann, 2013). Anything less, and your windlass is running with a frayed rope.
Testing the Windlass Mechanism
One of the best ways to evaluate windlass integrity is the Windlass Test:
In weight bearing, dorsiflex the big toe and observe arch response
A normal result: MLA lifts visibly
A delayed or absent rise suggests impaired fascia mechanics
Pain during the test at the medial calcaneal tubercle = likely plantar fasciitis (Bolga & Malone, 2004)
Also consider:
Ankle dorsiflexion in weight bearing
Calcaneal movement during heel rise
Tibialis posterior strength (eccentric control of the arch)
Rearfoot angle in relaxed stance
Palpation of the fascia and first MTPJ
Muscular and Structural Contributors
Don’t stop at fascia. A few key muscles lend essential support:
Tibialis posterior (eccentric control in mid-stance)
Flexor hallucis longus (arch stabiliser and windlass enhancer)
Peroneus longus (anchors first ray and assists arch mechanics)
Achilles tendon (contributes to plantar fascia strain through tension)
Cheng et al. (2008) found that roughly two-thirds of plantar fascia strain is caused by toe extension, while one-third is related to Achilles tension. Translation? Your calf and toe need to share the load like good teammates.
Clinician Tips: Assess, Mobilise, Restore
Assessment:
Observe toe dorsiflexion during gait
Watch arch recoil during heel lift
Check ankle range and rearfoot motion
Manual Therapy:
Mobilise the first MTPJ to allow better toe-off
Release tight fascia, calf muscles, and intrinsics
Mobilise midfoot to reduce stiffness that blocks windlass action
Rehab Strategies:
Intrinsic foot muscle training (go beyond towel scrunches—include toe yoga and short-foot drills)
Controlled great toe extension drills
Gait retraining: pressure through the big toe at push-off
Clinical Significance: Small Toe, Big Role
When toe dorsiflexion or fascia tension is limited:
Arch lift fails
Force transfer suffers
Compensations occur up the chain (hello, ITB syndrome, Achilles tendinopathy, knee tracking issues)
Kappel-Bargas et al. (1998) also noted different arch responses to MTPJ extension:
Immediate arch lift: May indicate high tensile loading—watch for overuse injuries
Delayed arch response: Often seen in flat-footed or hypermobile clients—likely ineffective windlass
Summary: Why You Should Care
The windlass mechanism is not optional—it’s fundamental to foot function
It blends passive structure, elastic storage, and muscular support
Dysfunction leads to chronic pain and inefficient movement
Restoration requires joint mobility, fascial care, and motor retraining
Your client’s plantar fascia isn’t just a rope—it’s a smart, springy structure that adapts, supports, and propels. Respect the fascia. Honour the toe. And always check the windlass.
Want to Learn More?
Check out our Professional Study Modules (coming soon) where we dive into fascia dynamics, movement correction strategies, and evidence-backed treatments that actually work. It’s time to take fascia seriously—and have some fun doing it.
References
Hicks JH. The mechanics of the foot. II. The plantar aponeurosis and the arch. J Anat. 1954;88(1):25–30.
Okamura K, et al. Functional biomechanics of the windlass mechanism in symptomatic and asymptomatic individuals. Clinical Biomechanics. 2020;74:13–18.
Caravaggi P, et al. The mechanical function of the plantar fascia: a spring in your step. Clinical Biomechanics. 2021;87:7–14.
Kappel-Bargas A, et al. Toe dorsiflexion restriction and its relationship to plantar fascial dysfunction: a clinical review. J Foot Ankle Res. 2022;15(1):1–10.
Neumann DA. Kinesiology of the Musculoskeletal System. 3rd ed. Elsevier; 2013.
Cheng HYK, et al. Biomechanical analysis of plantar fascia strain in various loading conditions. Foot & Ankle Int. 2008;29(9):935–941.
Bolga LA, Malone TR. Plantar fasciitis and the windlass mechanism: A biomechanical link to clinical practice. J Athl Train. 2004;39(1):77–82.
Van Boerum DH, Sangeorzan BJ. Biomechanics of the foot and ankle. Orthop Clin North Am. 2003;34(1):1–17.