Knee Pain Treatment Canberra — Long-Term Relief Through Biomechanics and Movement Therapy

Struggling with Knee Pain in Canberra?
Whether you’re a weekend runner, desk-bound professional, or parent constantly on the move — knee pain can stop you in your tracks. It’s one of the most common musculoskeletal complaints worldwide, affecting up to 25% of adults(Culvenor & Crossley, 2019).
But here’s the catch:
Your knee might not actually be the problem.
Most ongoing knee pain stems from how the entire lower limb moves — not from the joint itself.
At The Body Lab Canberra, I take a movement-first, evidence-based approach using functional biomechanics, pressure-plate gait analysis, and hands-on therapy to uncover the root cause and retrain the system, not just the symptom.
What Is Knee Pain, Really?
Knee pain isn’t just soreness — it’s a mechanical signal that load, alignment, or timing has gone wrong somewhere in the chain. It may appear as:
Sharp pain during running or squatting
Dull ache after sitting or walking
Stiffness or swelling around the patella
Difficulty climbing stairs or kneeling
When left unchecked, small movement faults can lead to cartilage wear, tendon overload, and even hip or spinal discomfort (Bennell et al., 2015).
Why Knees Start Complaining
🔁 Overuse or Repetitive Loading
Running, cycling, or repetitive squats can exceed the tendon’s ability to recover, leading to patellar tendinopathy or runner’s knee (Cook & Purdam, 2009).
🧩 Biomechanical Imbalances
Restricted ankle dorsiflexion, weak glutes, or pelvic asymmetry alter how forces travel through the knee. When the hip and foot stop sharing load, the knee becomes the middle-management scapegoat.
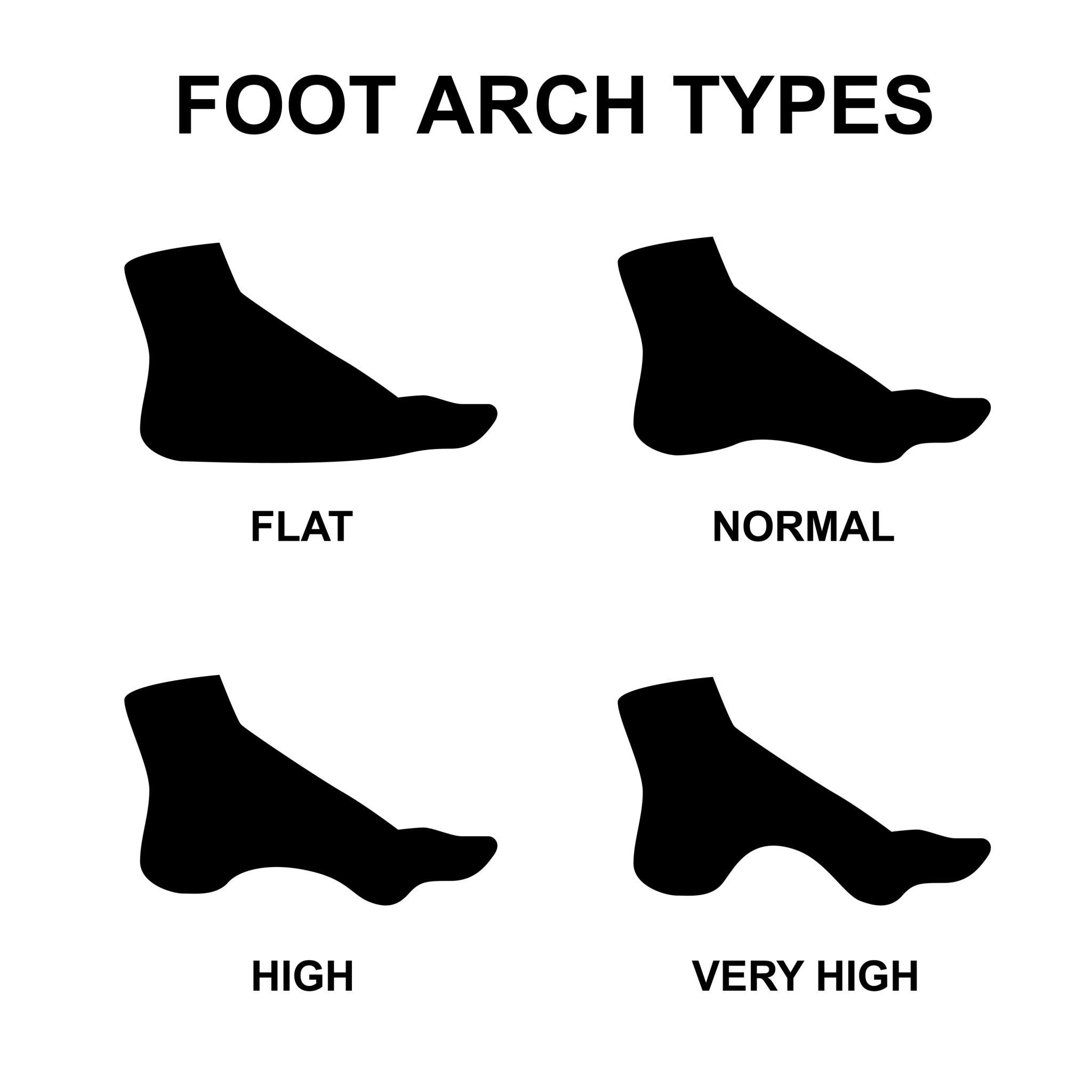
👣 Foot Mechanics and Gait Dysfunction
Flat feet, high arches, or stiff big toes distort tibial rotation and knee tracking. Studies show altered pronation–supination patterns directly influence patellofemoral stress (Noehren et al., 2012).
🦴 Arthritis and Age-Related Change
Osteoarthritis is common but not inevitable. Restoring joint mobility and neuromuscular control can significantly reduce pain and improve function (Skou et al., 2018).
Inside a Knee-Pain Session at The Body Lab
Every appointment follows a structured, research-informed sequence:
1️⃣ Comprehensive History and Movement Interview
We discuss your pain timeline, daily habits, previous injuries, and training load. Understanding context helps determine whether the issue is inflammatory, degenerative, or mechanical.
2️⃣ Pressure-Plate and 3D Gait Analysis
Canberra’s only FootWork Pro™ pressure system maps how you load the ground during walking and squatting.
It reveals asymmetries, timing delays, and over-dominant zones — data essential for identifying kinetic-chain errors.
3️⃣ Full-Body Biomechanical Assessment
I observe how your feet, knees, hips, and spine cooperate in three planes of motion.
This includes:
Closed-chain joint motion tests (tibia-femur rotation, pelvic shift)
Functional balance and single-leg stability
Range-of-motion testing for ankle, hip, and lumbar segments
4️⃣ Manual & Joint Mobilisation
Targeted releases improve glide and proprioception through the ankle mortise, fibular head, and patellofemoral joint.
Gentle myofascial and fascial-line work resets tension patterns (Wilke et al., 2016).
5️⃣ Movement Retraining
Once the system moves freely, we lock in change with tailored drills:
Foot tripod and arch-control activation
Glute–hamstring co-ordination patterns
Tibial rotation & hip-hinge sequencing
Dynamic single-leg balance
Each exercise is chosen to restore the body’s natural gait rhythm, not to isolate muscles in a vacuum.
6️⃣ Education and Take-Home Plan
You’ll leave knowing exactly why your knee hurts and how to move differently.
I email you a digital plan with video links, cues, and progressions — no generic rehab sheet.
The Research Behind This Approach
Movement retraining has been shown to reduce patellofemoral pain by up to 65% through altering hip and knee kinematics (Willy et al., 2012).
Foot-targeted interventions improve lower-limb alignment and reduce medial knee load (Hunt et al., 2011).
Neuromuscular exercise programs significantly outperform passive treatments for knee osteoarthritis (Skou et al., 2018).
Load-management education and progressive strength training reduce recurrence of tendon-related knee pain (Cook & Purdam, 2009).
Every Body Lab protocol integrates these findings into practical, real-world movement therapy.
How My Method Differs

Common Knee Conditions I Treat
Patellar & Quadriceps Tendinopathy
Iliotibial Band Syndrome (ITBS)
Patellofemoral Pain Syndrome
Meniscal Irritation or Degeneration
Ligament Sprains (ACL, MCL)
Osteoarthritis-related Knee Pain
Post-surgical Stiffness & Scar Tissue
Knee Pain from Foot or Hip Dysfunction
When Will My Knee Pain Improve?
Results depend on the cause and chronicity:
Acute overload: often resolves within 2–6 weeks.
Chronic dysfunction: typically improves 40–60 % within the first three sessions as mechanics normalise.
Arthritic knees: gain better range, less swelling, and improved gait efficiency within 6–10 weeks of structured retraining.
The earlier you address movement, the faster the recovery.
Ready to Fix Your Knee Pain for Good?
If you’re done masking pain and want a real, biomechanical solution — it’s time to move differently.
📅 Book a Comprehensive Knee Assessment
📞 Or call 0432 785 135 to speak with Riccardo.
📍 Clinic located in Ainslie — serving the greater Canberra region.
References Bennell, K.L. et al., 2015. Efficacy of exercise and education for knee osteoarthritis. Annals of the Rheumatic Diseases, 74(7), pp.1194–1200.Cook, J.L. & Purdam, C.R., 2009. Is tendon pathology a continuum? British Journal of Sports Medicine, 43(6), pp.409–416.Culvenor, A.G. & Crossley, K.M., 2019. Mechanisms and management of knee pain. BMJ, 364, l682.Hunt, M.A. et al., 2011. Foot motion and loading influence knee joint moments. Clinical Biomechanics, 26(1), pp.85–90.Noehren, B. et al., 2012. Lower extremity kinematics in runners with knee pain. Medicine & Science in Sports & Exercise, 44(5), pp.943–950.Skou, S.T. et al., 2018. Long-term effectiveness of exercise therapy in knee OA. Arthritis Care & Research, 70(12), pp.1757–1765.Wilke, J. et al., 2016. Fascia as a body-wide sensory network. Frontiers in Physiology, 7, p.8.Willy, R.W. et al., 2012. Patellofemoral pain and movement retraining. British Journal of Sports Medicine, 46(7), pp.407–413.