The Man in Thongs Who Showed Me Why So Many People End Up With Back Pain
Over the weekend, I posted two short social media videos showing a gentleman walking past from a side view at a kids’ sporting match. There was nothing particularly dramatic about it. No fancy gait lab, no treadmill, no reflective motion-capture markers stuck to his body like a low-budget sci-fi movie. Just a bloke in thongs walking across a sports field.
But honestly, it was one of the clearest examples of something I see constantly in clinic.
What struck me immediately was how little his body changed shape throughout the walking cycle. From heel strike through to mid-stance, his foot, ankle, knee, pelvis, and trunk essentially maintained the same overall posture. The system never really transitioned into a loading strategy. It simply stayed rigid and moved forward.
That might not sound like a big deal at first glance, but walking is supposed to be a constant process of shape change. Every step your body takes is a negotiation between gravity, momentum, force, balance, and energy transfer. Your joints are designed to subtly reposition themselves at different moments in the gait cycle so force can be absorbed, redistributed, and eventually pushed back into the ground efficiently.
When the body stops changing shape, something else has to absorb the force instead. More often than not, the lumbar spine becomes the poor sucker left doing everyone else’s job.
Walking Is a Force Management System
Most people think walking is simply “put one foot in front of the other and keep going.” Biomechanically, though, it is far more complex than that. Walking is one of the body’s primary force-management systems. Every step generates ground reaction force that travels upward through the foot, ankle, knee, hip, pelvis, and spine. Research from gait biomechanics pioneers like David A. Winter demonstrated decades ago that efficient walking depends on coordinated joint motion and the body’s ability to redistribute forces through constantly changing positions.
Healthy gait is not a rigid posture repeated over and over again. It is a controlled oscillation between loading and unloading, pronation and supination, absorption and propulsion.
What I observed in this gentleman was essentially one static strategy repeated throughout the entire walking cycle.
At initial contact, his ankle remained relatively plantarflexed, meaning the foot was tilted downward rather than allowing the ankle to dorsiflex and accept load. His knee remained extended and relatively stiff. His pelvis appeared anteriorly tilted, and the hip never really flexed into a position capable of helping absorb force. The entire lower limb behaved more like a rigid pole than an adaptable suspension system.
This matters because heel strike is supposed to begin the body’s loading response. We want to see the system yield slightly to incoming force. Not collapse, but adapt.

Initial Contact

Loading Phase

Mid-Stance

Terminal Stance
Ideally, at initial contact we would observe the ankle capable of dorsiflexion, a knee that is straight but adaptable, a pelvis able to orient posteriorly, and a hip joint flexed enough to help create an effective loading pattern. These positions allow the body to begin dissipating force rather than simply transmitting it upward.
Instead, this gentleman maintained essentially the same posture from heel strike all the way through mid-stance
Why the Loading Phase Matters So Much
The loading phase of gait is one of the most misunderstood parts of human movement. Many people have been taught that pronation is inherently bad, as though the foot flattening slightly is some kind of mechanical failure. In reality, pronation is one of the body’s primary loading strategies.
During loading response, the foot should become more adaptable. The arch lowers slightly, the ankle dorsiflexes further, the knee flexes, and the pelvis rotates and tilts to help absorb force. This creates what I often call a “loading shape.” The body essentially softens into the ground to manage incoming forces efficiently.
Research from Hamill and colleagues has consistently shown that walking generates significant ground reaction forces that must be distributed effectively through the kinetic chain. If the joints below fail to absorb those forces, the stress simply moves elsewhere.
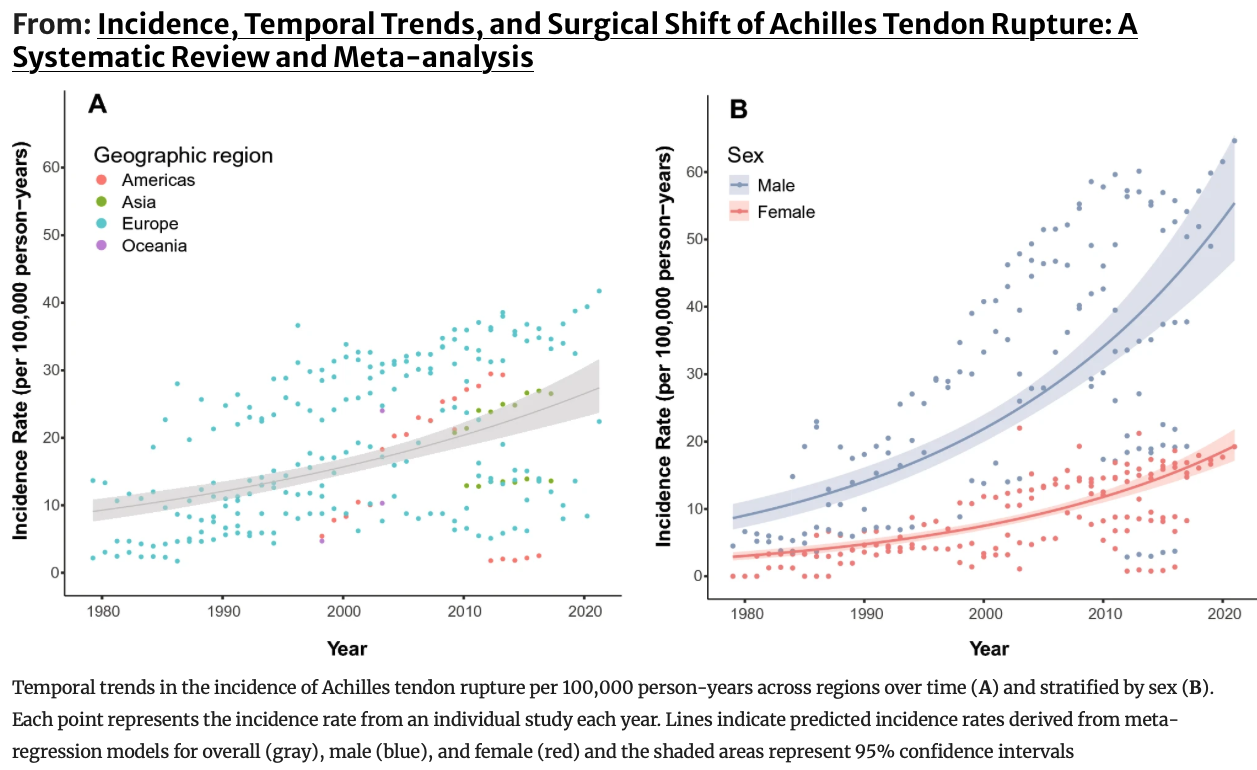
That “elsewhere” is often the lumbar spine, hips, knees, Achilles tendon, or plantar fascia.
The body is remarkably good at compensating in the short term. The problem is that compensation repeated thousands of times per day eventually becomes a long-term strategy. Over years, that strategy often becomes pain.
In this gentleman’s case, there was very little visible transition into a proper loading response. The ankle failed to dorsiflex effectively, the knee never meaningfully flexed, and the pelvis stayed relatively fixed. The system never truly entered the adaptable pronated position required for efficient force absorption.
Mid-Stance Should Reverse the Loading Strategy
Mid-stance is where the body should begin transitioning out of the loading phase and back toward propulsion. After moving into a more pronated, adaptable shape, the system should gradually recoil toward neutral. This becomes the beginning of supination and push-off.
Think of it like compressing and releasing a spring. The loading phase stores energy. Mid-stance begins reorganising that energy so the body can propel itself forward efficiently.
But here’s the problem: if the body never enters the loading phase properly in the first place, there is nothing meaningful to reverse out of. No elastic recoil. No spring. No efficient transfer of energy.
Instead, walking becomes a repetitive process of stiffness management.
This is something I see constantly in people with persistent back pain, hip tightness, calf tension, Achilles issues, plantar fasciitis, and chronic knee discomfort. The body simply loses its ability to transition between movement shapes.
The Long-Term Effects Go Beyond Pain
Most people only think about movement when something hurts. However, long-term reduction in joint motion affects much more than pain alone.
When joints stop articulating effectively, circulation often decreases. The calf muscles lose some of their pumping efficiency, which affects venous return back toward the heart. Muscles become less effective at assisting blood flow. Nerves can gradually become compressed or irritated through chronic positioning and stiffness. Breathing mechanics can also change because the pelvis, ribcage, and spine stop moving efficiently together.
Walking is one of the body’s major circulation systems. Your calf muscles are often referred to as the “second heart” because they help pump blood upward against gravity during movement. If the ankle, foot, and knee stop moving properly, that pumping action becomes less effective over time.
The body becomes mechanically quieter. Unfortunately, quiet bodies tend to become stiff bodies.
Movement Is Really About Timing
One of the biggest misconceptions in rehab is that movement problems are purely about strength or flexibility. In reality, timing is often the missing ingredient. The right motion has to occur at the right joint, at the right time, and in the right sequence.
A stiff ankle changes the knee. A knee that cannot flex properly changes the pelvis. A pelvis that stays anteriorly tilted changes the lumbar spine and ribcage. Everything is connected through force transfer and timing.
This is why detailed movement assessment matters so much. We are not simply asking whether something hurts. We are asking whether the joints can actually move through the motions required for efficient walking.
So How Do We Help?
The first step is determining whether the joints themselves are capable of movement. Sometimes the issue is not weakness at all. Sometimes the body has simply lost access to certain positions.
That means assessing:
foot articulation
ankle dorsiflexion
talocrural joint motion
tibial rotation
fibular mobility
femoral rotation
pelvic orientation
Then we look at how those joints behave during gait.
Can the ankle dorsiflex at heel strike? Does the heel tilt backwards effectively? Where is the restriction? During loading response, can the ankle continue dorsiflexing while the knee bends? Does the knee track efficiently? Does the foot actually adapt to the ground?
Then we assess rotational capacity. Can the ankle rotate? Can the tibia rotate? Can the pelvis reposition itself appropriately?
This is precisely why I use my Five Foot Assessment Tools system. The foot is not simply a foot. It is the starting point of force management for the entire body.
Assessment Is Often the Treatment
This is something I say regularly in clinic because it turns out to be true surprisingly often:
assessment itself becomes part of the treatment.
Once you become precise about joint motion, timing, sequence, and loading strategies, you stop guessing. Instead of randomly strengthening everything with a resistance band and hoping for the best, you begin restoring the exact movement strategy the body has lost.
Sometimes the changes occur remarkably quickly once the body rediscovers motions it has not used properly for years.
That gentleman at the sporting match probably had no idea any of this was happening. Most people do not. They simply think they are tight, getting older, or have a bad back.
But very often the body has simply stopped changing shape properly during walking.
And when the body loses its ability to adapt to force, the spine usually ends up paying the bill.
Reference
David A. Winter. Biomechanics and Motor Control of Human Movement. 4th ed. Wiley; 2009.
Hamill J, Knutzen KM, Derrick TR. Biomechanical Basis of Human Movement. 4th ed. Wolters Kluwer; 2015.
Perry J, Burnfield JM. Gait Analysis: Normal and Pathological Function. 2nd ed. Slack Incorporated; 2010.
Neumann DA. Kinesiology of the Musculoskeletal System. 3rd ed. Elsevier; 2017.
Blickhan R. The spring-mass model for running and hopping. J Biomech. 1989;22(11–12):1217–1227.
Clark KP, Weyand PG. Are running speeds maximized with simple-spring stance mechanics? J Appl Physiol. 2014;117(6):604–615.